
-
Understanding primary immunodeficiency (PI)
Understanding PI
The more you understand about primary immunodeficiency (PI), the better you can manage it. Learn about PI diagnoses and treatment options.
-
Living with PI

Living with PI
Living with primary immunodeficiency (PI) can be challenging, but you’re not alone—many people with PI lead full and active lives. With the right support and resources, you can, too.
-
Get involved

Get involved
Be a hero for those with PI. Change lives by promoting primary immunodeficiency (PI) awareness and taking action in your community through advocacy, donating, volunteering, or fundraising.
-
Advancing research and clinical care

Advancing research and clinical care
Whether you’re a clinician, researcher, or an individual with primary immunodeficiency (PI), IDF has resources to help you advance the field. Get details on surveys, grants, and clinical trials.

Key points
- Healthcare providers use laboratory testing to confirm or exclude primary immunodeficiency (PI) conditions.
- The clinical history (signs, symptoms, and specific infections) of the affected person are very important in determining which lab tests will be useful and informative in the medical evaluation.
- Healthcare providers increasingly use genetic testing in addition to lab tests to diagnose PI, but genetic testing has limitations because the specific genetic causes for the most common PI conditions are unknown.
- An experienced specialist who regularly sees patients with PI, like a clinical immunologist, is the best person to select and interpret lab tests for PI.
Making sense of laboratory test results
To figure out what laboratory test results mean, they must be compared to established reference ranges for that test. To define the reference range, the test maker tests a group of healthy people and looks at their results using statistics. Importantly, reference ranges can vary between laboratories based on local testing procedures and the populations used for reference testing. This variability means that tests done in different laboratories should be compared and interpreted with caution.
The 95% confidence interval is a common statistic that test makers use to define a test’s reference range. It is the range of values that includes 95% of the test results from healthy people (as in a bell curve). It is important to note that, when a test’s reference range is a 95% confidence interval, that means 5% of the tested healthy population has test values above or below the range, even though they are healthy.
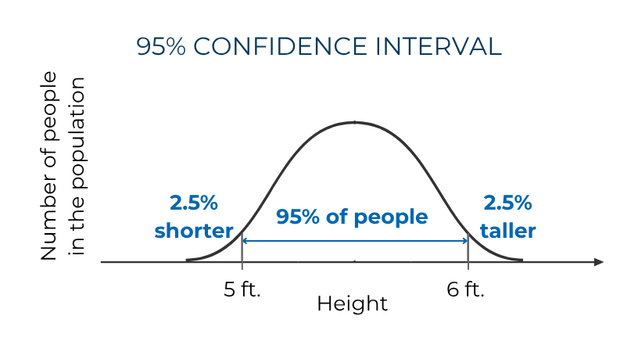
Think of height as an example. Someone one inch taller than 95% of healthy people does not necessarily have a growth disorder, and someone one inch shorter is not necessarily malnourished. By definition, 2.5% of healthy individuals will be shorter than the 95% confidence interval, and 2.5% will be taller.
The fact that 5% of otherwise healthy people fall outside a test’s reference range is important to remember when looking at results—a result outside of the reference range does not automatically mean there is a problem. How important a high or low laboratory test value is depends on context, especially the person’s medical history and the size of the difference from the reference range.
For laboratory tests looking at the immune system in children, the age of the group used to define a reference range is important because the immune system matures and changes as children grow. A test’s reference range for babies will be different than for toddlers or teenagers. As a result, all laboratory test results for children must be compared with age-matched reference ranges. If the laboratory reporting the results does not provide age-specific information, it is important to consult with a specialist who knows the published age-specific reference ranges for the test(s).
In addition, some laboratory tests may not be sensitive enough to detect a particular immune system problem. Results can also be affected by things like active infections or medications that suppress the immune system.
Complete blood count (CBC) with differential
One of the most common laboratory tests healthcare providers order is called a complete blood count (CBC). It measures someone’s platelets, hemoglobin, red blood cells, and white blood cells. If a healthcare provider orders a CBC with differential, the laboratory does additional analysis to measure the different kinds of white blood cells, including neutrophils, lymphocytes (which are B cells, T cells, and natural killer (NK) cells together), monocytes, basophils, and eosinophils.
Several CBC with differential results can be helpful for diagnosing PI, including:
- Absolute lymphocyte count (ALC), which measures the total number of B cells, T cells, and NK cells.
- Absolute neutrophil count (ANC), which measures the number of neutrophils.
- Red blood count (RBC), which measures the number of red blood cells.
- Hemoglobin (Hb), which measures the amount of the protein that carries oxygen within red blood cells from the lungs to other parts of the body.
- Platelet count (PLT), which measures the number of a tiny type of blood cell fragment called platelets that help form blood clots.
Low numbers of lymphocytes (lymphopenia) can point to T cell problems since 75% of lymphocytes in the bloodstream are T cells. Before newborn screening, a CBC with differential was the first test healthcare providers ordered for babies suspected of having severe combined immune deficiency (SCID). Note that some people with an ALC within the reference range still have a low number of T cells or T cells that don’t work properly. This means that an ALC within the reference range does not rule out T cell problems.
Likewise, low numbers of neutrophils (neutropenia) can point to a problem with neutrophil immunity or to other PIs like CD40 ligand deficiency. Because neutrophil numbers vary over time and in response to infections, healthcare providers looking for PI usually look for consistently low ANCs over time.
Both low ALC and low ANC have to be followed up with other tests to diagnose PI because there are many other reasons someone might have low values.
Low RBC and Hb levels can point to anemia, which can have many causes including a chronic condition or iron deficiency. In some forms of PI like common variable immune deficiency (CVID), autoimmune hemolytic anemia (AIHA) is a serious complication in which the immune system destroys its own red blood cells. Healthcare providers have to do additional testing to determine if low RBC and Hb levels are caused by AIHA. If a person has AIHA, providers may do additional immune system testing to find out whether it is a symptom of PI or not.
Low PLT levels (thrombocytopenia) can also be a complication in some types of PI when the immune system attacks platelets (immune thrombocytopenic purpura; ITP). ITP can happen in CVID and other PIs like autoimmune lymphoproliferative syndrome (ALPS). People with Wiskott-Aldrich syndrome (WAS) have thrombocytopenia but with low mean platelet volume (MPV), which means that their platelets are also small. Healthcare providers have to do additional tests to find out if someone’s thrombocytopenia might be a symptom of PI.
It is important to remember that none of the results from a CBC with differential can diagnose PI alone. They must be followed up with other, more specific tests. In addition, CBC results within the reference ranges do not rule out PI either.
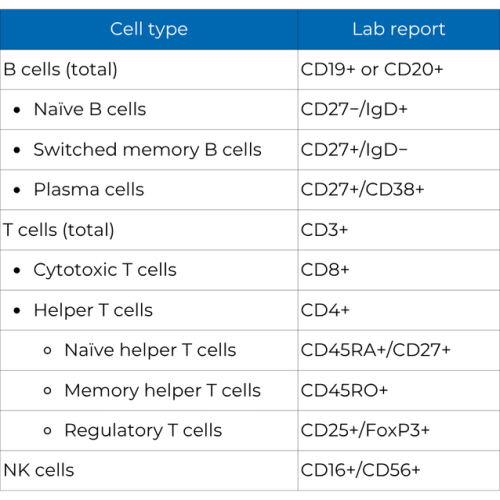
How lab reports label immune system cells
Cell subsets are indented under the larger cell type group they belong to. Depending on the lab, these subsets may be labeled with all of the markers used to identify them or just the markers that are unique to that subset. For example, cytotoxic T cells may be labeled "CD3+/CD8+" or just "CD8+."
Testing neutrophils
Healthcare providers might order a test called a blood smear if they think there may be a problem with someone’s neutrophils. For a blood smear, the laboratory takes a drop of blood and spreads it across a microscope slide, then looks at the cells for any visible problems. A careful review of the blood smear is important to rule out certain conditions that are associated with problems in the structure of neutrophils. Specific abnormal neutrophil features can occur in rare PIs such as Chediak-Higashi syndrome, but other structural changes may point to nutritional deficiencies, bone marrow disorders, or autoimmune conditions.
If initial tests of neutrophil numbers and appearance don’t find a problem, testing then focuses on two possible types of PI: chronic granulomatous disease (CGD) and leukocyte adhesion deficiency (LAD). People with these disorders have either typical or high neutrophil numbers, so their ANC will be either in or above the reference range. Each of these disorders has distinctive signs and symptoms that can help healthcare providers choose the appropriate testing.
Laboratory testing to diagnose CGD looks at how well a person’s neutrophils make reactive oxygen, a group of chemicals these white blood cells use to kill certain bacteria and fungi. This process, called the oxidative burst, can be measured using several different methods. The most common and reliable method uses flow cytometry to measure the oxidative burst of activated neutrophils using a dye called dihydrorhodamine (DHR). The DHR test is more sensitive than other tests and can point to whether someone has X-linked or autosomal recessive CGD [2]. It can also help identify carriers of CGD. Once the DHR test shows that someone has CGD, healthcare providers will order genetic testing to confirm which type of CGD the person has.
Laboratory testing for the most common form of LAD, called LAD1, uses flow cytometry to look for CD18/CD11a on the surface of neutrophils and other white blood cells. When this protein is missing, neutrophils can’t move to sites of infection, so there is an increased number of these cells in the person’s bloodstream.
Testing the complement system
PIs affecting the complement system typically cause recurrent infections with specific types of sugar-coated bacteria like Streptococcus pneumoniae or Neisseria meningitidis, or serious autoimmune issues, most often systemic lupus erythematosus (SLE). If a healthcare provider thinks someone has a complement system problem, they may order an initial test called the total hemolytic complement assay (CH50). This test measures the combined activity of the nine proteins in the classical complement pathway in a person’s blood. Someone who lacks or has a problem with any one protein in the pathway will have almost no measurable complement in the CH50 test. However, the test does not tell healthcare providers which complement protein is missing or not working.
The AH50 test, which is similar to the CH50 test, uses a blood sample to measure how well the alternate complement pathway works. There are some very rare PIs that affect proteins that are part of the alternate complement pathway but not in the classical pathway. In these cases, the person would have CH50 results within the reference range, but would not have measurable complement with the AH50 test.
Because the classical and alternative complement pathways share some proteins, the AH50 test can help narrow down which complement protein is missing or doesn’t work in someone who does not have measurable CH50 results [3]. Specialized laboratories can do additional testing to find out exactly which complement protein is affected.
Testing other parts of the innate immune system
Laboratory tests can also measure parts of the innate immune system aside from neutrophils and the complement system. These tests are typically used only in very specific situations when a person’s clinical history and symptoms suggest a very rare PI. For instance, determining the number and activity of natural killer (NK) cells (CD16+/CD 56+) can help diagnose a person with frequent and severe recurring herpesvirus infections. Healthcare providers might test the function of various cell surface proteins such as toll-like receptors (TLRs) if someone has severe, recurrent invasive infections and the usual comprehensive testing for PI fails to identify a specific cause or diagnosis.
This page contains general medical and/or legal information that cannot be applied safely to any individual case. Medical and/or legal knowledge and practice can change rapidly. Therefore, this page should not be used as a substitute for professional medical and/or legal advice. Additionally, links to other resources and websites are shared for informational purposes only and should not be considered an endorsement by the Immune Deficiency Foundation.
Adapted from the IDF Patient & Family Handbook for Primary Immunodeficiency Diseases, Sixth Edition.
Copyright ©2019 by Immune Deficiency Foundation, USA.
Sign up for updates
Receive news and helpful resources to your cell phone or inbox. You can change or cancel your subscription at any time.
