
-
Understanding primary immunodeficiency (PI)
Understanding PI
The more you understand about primary immunodeficiency (PI), the better you can manage it. Learn about PI diagnoses and treatment options.
-
Living with PI

Living with PI
Living with primary immunodeficiency (PI) can be challenging, but you’re not alone—many people with PI lead full and active lives. With the right support and resources, you can, too.
-
Get involved

Get involved
Be a hero for those with PI. Change lives by promoting primary immunodeficiency (PI) awareness and taking action in your community through advocacy, donating, volunteering, or fundraising.
-
Advancing research and clinical care

Advancing research and clinical care
Whether you’re a clinician, researcher, or an individual with primary immunodeficiency (PI), these resources will help you advance the field. Get details on surveys, grants, and clinical trials.

Key points:
- Genetic testing is an important part of diagnosing many primary immunodeficiencies (PIs) and can help your healthcare providers develop a personalized treatment or management plan for your condition.
- In general, genetic testing for PI does not provide results for other genetic conditions unless they are part of the ACMG recommended secondary findings list.
- Genetic testing can help identify people who do not yet have symptoms of PI, including family members at risk of developing PI.
- If genetic testing does not lead to a genetic diagnosis, the results can be reanalyzed every few years as new information becomes available.
What is genetic testing?
Primary immunodeficiencies (PIs), also known as inborn errors of immunity (IEIs), are conditions caused by changes in a person’s DNA. Four nucleotides make up DNA: adenine (A), thymidine (T), guanine (G), and cytosine (C). The order of these nucleotides, or the DNA "sequence," is a code. This code contains instructions for making proteins, cells, and organs, similar to how a specific order of alphabet letters form words, sentences, and paragraphs. Each stretch of DNA that codes for a particular protein or other molecule is called a gene.
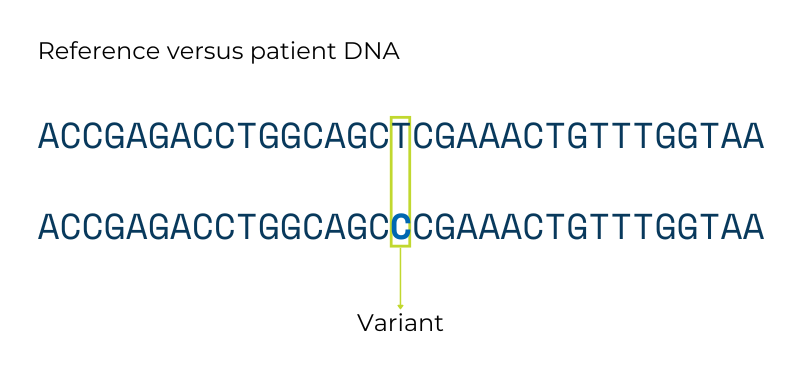
Unless two people are identical twins, their DNA sequences have millions of differences across genes, which are known as genetic ‘variants.’ These genetic variants between people lead to differences in all kinds of traits like height and blood type. Genetic testing looks for these variants. Most variants do not really change the overall genetic instructions and do not cause genetic disorders. However, some variants change the instructions a lot, and those types of variants can cause genetic conditions like PI.
Healthcare providers use genetic testing to look for gene variants that are likely to cause PI symptoms. They can use genetic testing to confirm a diagnosis that was made based on clinical symptoms or blood test results, or to find a more precise diagnosis if a person’s symptoms or test results don’t point to one particular disorder. When there is a strong family history of PI, genetic testing can also determine if someone who does not yet have symptoms is at high risk for developing PI.
Results from genetic testing can not only provide a genetic diagnosis, but can also affect treatment and clinical management. For example, there are now some medications that are targeted to specific genetic PIs. Genetic testing can also be important for family planning decisions, and knowing whether relatives are at risk of PI. For example, several genetic variants that are passed down in families in different ways cause chronic granulomatous disease (CGD). Knowing which variant a person with CGD has and how it’s passed down is important for family planning and understanding who else in the family is at risk.
Genetic testing is a powerful tool. However, it’s important to understand that all of us have differences in our DNA compared to other people, and not all genetic variants are harmful or cause medical conditions. Most genetic variants are like the American versus British spellings for words like gray—the variant doesn’t change how the gene works. In addition, the genetic cause of some of the most common PIs, such as common variable immune deficiency (CVID), remains unknown, and some patients who have genetic testing will not receive a genetic diagnosis.
Types of genetic tests
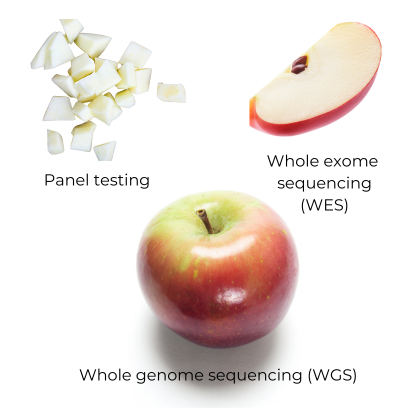
Generally, there are four types of genetic testing commonly used to diagnose PI: panel testing, whole exome sequencing (WES), whole genome sequencing (WGS), and chromosomal microarray (CMA). The first three use the same type of technology, which reads a person’s DNA sequence. The CMA test does not specifically look at the DNA sequence but detects when stretches of DNA are missing or duplicated. These duplicated or deleted stretches may contain parts of a gene, one or more whole genes, or important DNA sequences for controlling when genes are turned on or off.
The different types of testing can all provide a PI diagnosis, but they differ in the numbers of genes tested and type of genetic information they provide. In addition to your healthcare professional, you may meet with a genetic counselor or a physician who specializes in genetic disorders (geneticist) to discuss genetic testing. Genetic counselors are trained to help you understand testing options and genetic conditions. With any genetic testing, the person getting tested and the healthcare provider ordering the test should understand the test’s limitations.
There are some situations where your healthcare provider may order a type of genetic test that is different from the ones listed here. For example, one of the more common forms of CGD can only be detected by an older but still very useful method of genetic testing called Sanger sequencing that looks at one gene at a time [1].
Genetic testing has unique risks
Information from genetic testing is more sensitive than other types of medical information. In 2008, Congress passed the Genetic Information Non-discrimination Act (GINA) [6]. GINA bans employers and health insurance companies from using genetic information in employment or coverage decisions. GINA also clarifies that genetic information is a type of medical information that falls under the Health Insurance Portability and Accountability Act (HIPAA) privacy rules.
However, GINA has limits. For example, the military does not have to follow the employer rules and can use genetic information in employment decisions. In addition, genetic information can legally be used to determine if someone qualifies for life or long-term care insurance. Law enforcement can also force healthcare providers or testing laboratories to share genetic information from medical records, which could link someone or their relatives to a crime [7].
Some states have passed additional genetic information privacy laws that are broader than GINA [8]. For example, a 2021 Connecticut law makes it illegal for companies to use genetic information for coverage decisions for many types of insurance.
In addition to being used in ways you may not agree with, your genetic testing results can reveal information you may not be prepared for. This information can range from learning that you have a genetic condition aside from PI (secondary findings) to learning that the people who raised you are not your biological parents. Genetic counselors can help people understand and think through these possibilities before undergoing genetic testing.
Reanalyzing genetic testing data
Unlike other types of medical tests, your genetic sequence does not change over time. That means that your raw genetic data can be reanalyzed as labs update their lists of PI-related or immune system-related variants and reclassify VUSs. Be sure to retain a copy of your test results and consider contacting the provider who ordered the test or the testing lab to request updates every couple of years if your condition remains undiagnosed. Each year, there are more than a dozen new genetic PIs identified by researchers and reanalyzing your genetic testing to stay up to date is important.
Carrier testing for autosomal or X-linked PIs
Panel testing, WES, and WGS can identify gene variants not only in individuals with PI but in their unaffected family members. In cases of a family history of autosomal recessive or X-linked PI, family members, such as the parents or siblings of the person with PI, can undergo carrier testing. Carrier testing determines if someone ‘carries’ one copy of a gene variant linked to PI. In most cases, carriers do not themselves have PI symptoms, although there are exceptions, such as women who carry the variant that causes X-linked chronic granulomatous disease (CGD) and Wiskott-Aldrich syndrome (WAS).
People who are considering becoming parents should seek information from healthcare providers such as pediatricians, genetic counselors, immunologists, and obstetricians on current medical advances relating to the PI of concern. Families with a known history of PI should strongly consider genetic counseling, as it allows for early detection, diagnosis, and treatment.
Talk with your provider
Here are a few questions to ask your healthcare provider about genetic testing:
- Have I had a genetic test?
- If I have previously had a genetic test that did not result in a genetic diagnosis (i.e., results were indeterminate or negative), should I consider retesting or reanalysis?
- Could the results of a genetic test alter my treatment or management plan, or inform family planning decisions?
- Why do you/do you not recommend genetic testing for me?

Sponsored, free genetic testing
There is a sponsored, no-charge genetic testing program available for people who are suspected of having APDS (activated PI3K delta syndrome).
Talk to your provider to determine if you meet the criteria to qualify for this genetic testing program.
navigateAPDS includes pre- and/or post-testing genetic counseling services that provide support to help your family better understand the testing process, what to anticipate in terms of results, and what information is needed by your physician.
This program is available to patients in the U.S. and Canada who meet any two or more of the following bulleted criteria:
Clinical features:
- Bronchiectasis.
- Lymphadenopathy for greater than one month.
- Chronic hepatomegaly or chronic splenomegaly.
- Severe, persistent, or recurrent Herpesviridae infections (e.g., EBV, cytomegalovirus).
- Enteropathy.
- Lymphoma at 0-25 years—meets both eligibility criteria.
- Lymphoma at ≥ 26 years of age—requires second eligibility criteria.
Lab tests:
- Elevated levels of immunoglobulin M (IgM).
- Increased number of follicular helper T cells.
- Reduced number of naïve B cells.
History:
- Common variable immune deficiency (CVID) phenotype or direct family member with CVID phenotype.
- Relative with PIK3CD or PIK3R1 genotype (first or second degree)—meets both eligibility criteria.
This page is supported by

This page contains general medical and/or legal information that cannot be applied safely to any individual case. Medical and/or legal knowledge and practice can change rapidly. Therefore, this page should not be used as a substitute for professional medical and/or legal advice. Additionally, links to other resources and websites are shared for informational purposes only and should not be considered an endorsement by the Immune Deficiency Foundation.
Adapted from the Patient & Family Handbook for Primary Immunodeficiency Diseases, Sixth Edition.
Copyright ©2019 by Immune Deficiency Foundation, USA.
Sign up for updates
Receive news and helpful resources to your cell phone or inbox. You can change or cancel your subscription at any time.
