
Transient hypogammaglobulinemia infancy
When it takes longer than expected for a baby to make their own IgG antibodies, they may have transient hypogammaglobulinemia of infancy (THI).
The more you understand about primary immunodeficiency (PI), the better you can manage it. Learn about PI diagnoses and treatment options.

Living with primary immunodeficiency (PI) can be challenging, but you’re not alone—many people with PI lead full and active lives. With the right support and resources, you can, too.

Be a hero for those with PI. Change lives by promoting primary immunodeficiency (PI) awareness and taking action in your community through advocacy, donating, volunteering, or fundraising.

Whether you’re a clinician, researcher, or an individual with primary immunodeficiency (PI), IDF has resources to help you advance the field. Get details on surveys, grants, and clinical trials.

When it takes longer than expected for a baby to make their own IgG antibodies, they may have transient hypogammaglobulinemia of infancy (THI).
Newborn babies are unable to make their own IgG antibodies. Instead, babies rely on the IgG that passes through the placenta to them from their mother during the last three months of pregnancy. This IgG is important in protecting babies against infections. The other immunoglobulins, IgA, IgM, and IgE, do not cross the placenta.
When IgG levels are checked in a newborn, the levels reflect the IgG received from the mother. Babies born early, or prematurely, have less time to receive IgG from their mothers, so they may have lower IgG levels. Gradually, the baby's own immune system matures and begins to make its own IgG. Sometimes it takes longer than expected for children to make their own sufficient levels of IgG. This is called transient hypogammaglobulinemia of infancy (THI).
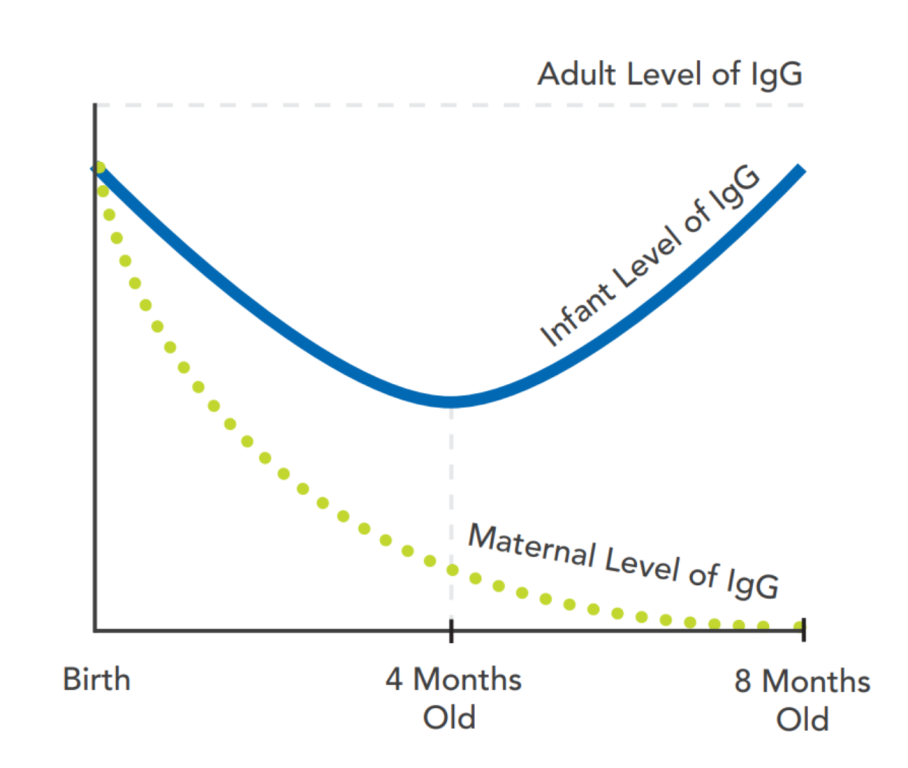
All babies have a period of low IgG, or hypogammaglobulinemia, when the levels of the mother's IgG are decreasing and the baby's production of IgG is increasing. This generally occurs when babies are 3-6 months of age and may be more pronounced in premature infants.
When low IgG levels persist past 6 months of age, THI may be suspected. It has been estimated that as many as one in 1,000 children have THI. The true frequency of THI is unknown because immunoglobulins are not routinely checked in healthy children. For this reason, THI may be underdiagnosed. THI has been reported around the world. Both males and females are affected, though males appear to be affected about twice as often as females.
The cause of THI is unknown, but it is thought to be due to B cells (the cells that make antibodies) taking longer to mature than normal.
Some children with THI have no symptoms at all, while others have recurrent infections beginning in infancy. Asymptomatic children with THI may come to medical attention due to a family history of immune system problems.
In children with symptoms, recurrent upper respiratory tract infections are commonly seen, especially ear infections. Lower respiratory tract infections, such as bronchitis and pneumonia, can also occur. More severe infections affecting the bloodstream, brain, and gastrointestinal (GI) tract have been reported but are rare. If severe infections occur, it is important to consider other types of immunodeficiency as a possible cause. Infections in children with THI usually start to improve by age 2. Most children with THI have normal growth and development.
While THI may be suspected in an infant, the diagnosis can only be made once IgG levels have normalized, showing that the low level was temporary and not the result of another type of immunodeficiency. In other words, THI can only be officially diagnosed looking back over time.
The criteria for diagnosing THI include an IgG level that is lower than 95% of children of similar age (at least two standard deviations below the average level) when measured on at least two separate occasions. Other immunoglobulins, including IgA and IgM, might be normal or low in infants with THI.
Other immunodeficiencies must be ruled out prior to making the diagnosis. When the IgG is very low, or when all immunoglobulins are low, an alternate diagnosis should be considered. There are no specific findings on physical examination that help make the diagnosis of THI.
The evaluation should include checking antibody levels (titers) to things against which the child has been previously vaccinated, such as tetanus and pneumococcal vaccines. Most children with THI are able to make antibodies to vaccines. However, if vaccine titers are low, a booster dose of the vaccine may be given and antibody levels measured again after 4-6 weeks to evaluate the immune response. Immune memory may be evaluated by rechecking the vaccine antibody levels again in six months. If a child does not make antibodies to vaccines, consultation with an immunologist is indicated.
A complete blood count (CBC) with differential to check the numbers of white blood cells, especially the lymphocytes, is important in the work-up of THI. If lymphopenia, a low number or percent of lymphocytes, is present along with low IgG levels, additional studies will be necessary and consultation with an immunologist is warranted. This is because low lymphocyte numbers are not typically seen in THI and may be a sign of another type of PI. Additional reasons for consultation with an immunologist are severe or persistent infections, unusual infections, poor growth, chronic diarrhea, or IgG levels that do not improve over time.
It is important to rule out other causes of low IgG during the evaluation, including B cell defects (such as X-linked agammaglobulinemia) and combined T and B cell defects (such as severe combined immunodeficiency). In addition, it is important to rule out loss of IgG as a possible cause of a low IgG level. In THI, the IgG is low because the infant has trouble making IgG, which is a production problem. In contrast, some infants make normal levels of IgG but quickly lose it, such as infants with various gastrointestinal, heart, or kidney diseases.
Asymptomatic children with THI do not require treatment, but they still require monitoring until it is demonstrated that their IgG level has normalized and the child can make and maintain protective responses to vaccinations. For children with symptoms, the goal of treatment is to prevent infection. It is important to adhere to good hand hygiene and limit contact with sick individuals to reduce the risk of infection transmission.
In children who have frequent or severe bacterial infections, antibiotics are sometimes given prophylactically for prevention. Rarely, in those with recurrent or severe infections who continue to have infections even while receiving antibiotic prophylaxis, immunoglobulin (Ig) replacement therapy has been selectively used. However, the vast majority of children with THI do not require Ig replacement therapy.
Based on studies, it does not appear that using Ig replacement therapy prolongs the natural course of THI, but it is important to note it will delay further work-up. This is because when immunoglobulins and specific antibody levels are measured in someone receiving immunoglobulin replacement therapy, the IgG and antibody response levels reflect the amount of antibody in the Ig product, as well as any the child’s immune system is making. A period of 4-6 months off Ig replacement therapy is necessary before the child's own immunoglobulin levels and vaccine titers can be checked accurately. Generally, this assessment off of Ig replacement is done during the spring and summer months, after the flu and respiratory virus season.
Children who have low IgG levels should be closely followed, because low IgG can increase the risk for infections. Monitoring includes checking immunoglobulin and specific antibody levels, tracking growth, and evaluating for other possible causes of low IgG. The expectation is that IgG levels will normalize between 2-5 years of age.
If monitoring reveals persistently low immunoglobulin levels and/or low responses to vaccines, a different diagnosis should be considered. Some children initially suspected to have THI are later diagnosed with another antibody disorder such as common variable immune deficiency (CVID) or specific antibody deficiency when their THI does not resolve. Careful monitoring is important for this reason.
Until it is demonstrated that the child has normal production of antibodies, live viral vaccines, such as rotavirus, MMR, and chickenpox, should not be given. If a child has an impaired response to these vaccines, it is possible to contract the illness after vaccination.
This page contains general medical and/or legal information that cannot be applied safely to any individual case. Medical and/or legal knowledge and practice can change rapidly. Therefore, this page should not be used as a substitute for professional medical and/or legal advice. Additionally, links to other resources and websites are shared for informational purposes only and should not be considered an endorsement by the Immune Deficiency Foundation.
Adapted from the IDF Patient & Family Handbook for Primary Immunodeficiency Diseases, Sixth Edition.
Copyright ©2019 by Immune Deficiency Foundation, USA
Receive news and helpful resources to your cell phone or inbox. You can change or cancel your subscription at any time.


