
-
Understanding primary immunodeficiency (PI)
Understanding PI
The more you understand about primary immunodeficiency (PI), the better you can manage it. Learn about PI diagnoses and treatment options.
-
Living with PI

Living with PI
Living with primary immunodeficiency (PI) can be challenging, but you’re not alone—many people with PI lead full and active lives. With the right support and resources, you can, too.
-
Get involved

Get involved
Be a hero for those with PI. Change lives by promoting primary immunodeficiency (PI) awareness and taking action in your community through advocacy, donating, volunteering, or fundraising.
-
Advancing research and clinical care

Advancing research and clinical care
Whether you’re a clinician, researcher, or an individual with primary immunodeficiency (PI), IDF has resources to help you advance the field. Get details on surveys, grants, and clinical trials.

Key points:
- The gastrointestinal (GI) tract and liver can be affected by autoimmunity, inflammation, infection, and, sometimes, cancer in people with primary immunodeficiency (PI).
- The type of PI a person has influences how common or rare particular GI and liver problems are.
- GI and liver infections, autoimmunity, and inflammation can cause permanent organ damage and increase cancer risks, so it is important to seek care from providers experienced in diagnosing and managing these complications.
- It is important to remember that not all signs and symptoms of GI or liver disease are due to the PI, so providers should perform a thorough workup just as they would for someone without PI.
The digestive system, also known as the gastrointestinal (GI) tract, includes all the organs from your mouth to your anus. This system is responsible for taking in food, breaking it down to get nutrients, and getting rid of solid waste.
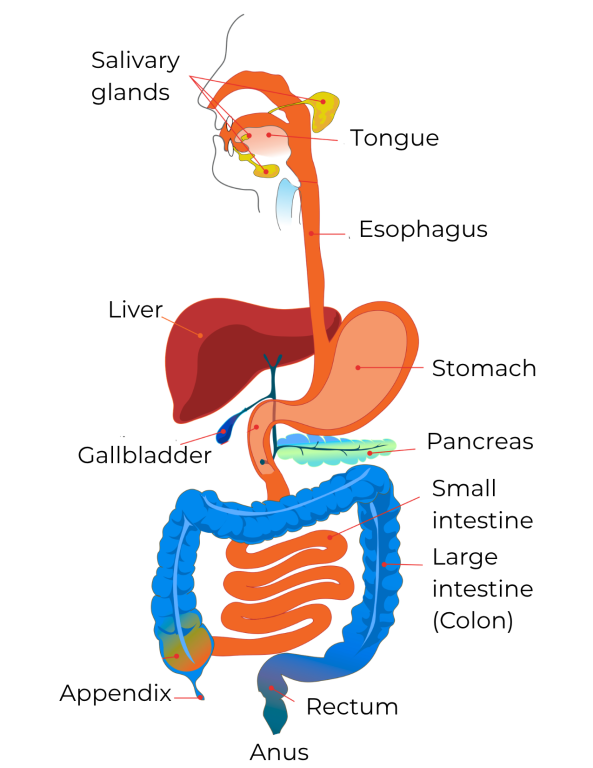
Here’s how the digestive system works:
- The mouth starts the process of breaking down food by chewing and mixing it with saliva, which has proteins that chemically digest the food.
- The esophagus is a muscular tube that moves the chewed food to the stomach. It also has a specialized muscle at its end to prevent stomach contents from getting back into the esophagus.
- The stomach further grinds up the food and continues chemical digestion.
- The food then goes to the small intestine, where it mixes with bile (from the liver) and more digestive proteins (from the pancreas) to be broken down even more.
- Nutrients are then absorbed through the wall of the small intestine into the bloodstream.
- Finally, the remaining waste passes into the colon (also known as the large intestine or bowel), where fluid is absorbed back into the body and stool is formed to be eliminated through the anus.
The liver is part of your digestive system and does many important things to keep your body working properly. Some of the most important jobs of the liver are:
- Breaking down nutrients absorbed by your intestines.
- Making important blood proteins, like clotting factors.
- Breaking down certain medications.
- Cleaning waste out of your blood.
- Getting rid of this waste through bile.
The GI tract has the largest number of immune system cells in the body and is one of the most frequent places that the immune system comes in contact with germs and other substances. Because of this, the digestive system is a common place to have symptoms related to primary immunodeficiency (PI), including infections, autoimmunity, inflammation, and, rarely, cancer.
Sometimes healthcare providers refer to GI conditions by the organ(s) that are affected:
- Hepatitis (liver).
- Gastritis (stomach).
- Pancreatitis (pancreas).
- Cholangitis (bile duct).
- Cholecystitis (gallbladder).
- Enteritis (small intestine).
- Colitis (large intestine).
These ‘-itis’ terms mean inflammation, but they do not reveal whether an infection or something else is causing the inflammation. The symptoms across different types of GI conditions can be similar, so it's important to get checked out and properly diagnosed. Your healthcare provider may refer you to a GI specialist (gastroenterologist) or a liver specialist (hepatologist). Early diagnosis and treatment can help prevent long-term problems and organ damage.
Many bacteria and other ‘good’ germs, such as viruses and fungi, live throughout the digestive system, with the highest numbers in the colon. As a group, they are called the gut microbiome. The gut microbiome acts almost as another organ within the GI system. Which germs are part of your gut microbiome and in what relative amounts affects:
- How your food gets broken down and what nutrients are available for your body to use (metabolism).
- Which chemical signals might move from your gut to your brain and nervous system.
- How active your immune system is, both within the GI system and in other parts of your body.
Microbiome problems can cause or worsen GI conditions. The condition of the gut microbiome may need to be considered when checking for digestive problems in people with PI.
Finally, it's important to remember that not everyone with PI has GI problems, and if they do, their GI problems may not always be directly caused by PI.
Cancer
Cancer in the digestive system can develop from either chronic infections or from chronic inflammation or autoimmunity. People with PIs that include an increased risk of lymphoma in general can develop intestinal lymphoma, which is when white blood cells grow and divide out of control, starting in the intestines. People with CVID or XLA can also develop gastric adenocarcinoma, which is the most common type of stomach cancer, either from chronic H. pylori infection or from autoimmune atrophic gastritis [36,37]. Since many of the GI conditions linked to PI are risk factors for GI cancer, it’s important to get diagnosed and treated as soon as possible if you have GI symptoms.
Diagnosing digestive system and liver conditions
Diagnosing GI conditions in people with PI often requires multiple steps. These steps include a physical exam, imaging tests, and laboratory blood and stool tests. For people with PI who have significant digestive symptoms, it is important to involve a gastroenterologist or hepatologist to help with diagnosis and to guide treatment.
During a physical exam, healthcare providers may look for mouth or anal sores, enlarged lymph nodes in the neck, armpits, or groin, stomach tenderness, fluid in the belly (ascites), an enlarged or tender liver and spleen, cracks around the anus, unintentional weight loss, and, in children, poor growth (sometimes called failure to thrive).
Signs and symptoms like general abdominal pain, changes in bowel habits, bloating, and upset stomach, as well as bleeding from the upper or lower GI tract, most often cannot be diagnosed without further tests.
If your healthcare provider thinks you have a GI infection, they will send stool samples to the laboratory to be tested, cultured, or stained and viewed under a microscope. These tests look for bacteria, parasites, viruses, or other germs that could be causing GI symptoms.
Other tests that healthcare providers use to diagnose GI or liver problems include:
- Upper endoscopy, where the provider introduces a camera on the end of a small flexible tube (endoscope) through the mouth into the GI tract to look at the esophagus, stomach, and upper small intestine.
- Colonoscopy, where the provider introduces an endoscope into the anus to look at the anus, rectum, colon, and the end of the small intestine.
- Percutaneous liver biopsy, where the provider removes a small piece of liver tissue (liver biopsy) by inserting a needle through the skin into the liver.
All of these tests are done with appropriate anesthesia. The endoscopic procedures check the gut lining for visible problems. They also allow the provider to take samples of the gut's contents and tissue samples (biopsies) for a specialist who looks at and tests body tissues for diseases (pathologist) to examine under a microscope. A pathologist will also examine any liver biopsies for signs of liver problems.
Other GI imaging tests include:
- Double balloon endoscopy (also known as push-and-pull endoscopy), which uses a much longer scope to look at the entire GI tract, specifically parts of the small intestines that regular endoscopy or colonoscopy can’t reach.
- Video endoscopy, which involves swallowing a pill-sized camera that takes pictures as it travels through the digestive system.
- X-rays of the belly or intestines.
- Ultrasounds of the belly or liver and bile ducts.
- Computerized tomography (CT) scans of the belly after swallowing dye (CT with contrast).
Laboratory tests for digestive system problems start with a complete blood count (CBC) and a stool test to check for blood loss, infection, protein loss, pancreatic function, or inflammation in the stomach or intestines. The tests a provider orders are guided by the types of symptoms the person has. The healthcare provider may also do additional blood tests to measure inflammation throughout the body like C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). These two tests will be high when there is an infection or inflammation, including autoimmune inflammation, in the body.
Blood tests for albumin and pre-albumin levels provide a general sense of a person's nutritional status. Low albumin levels can indicate that the liver is having trouble making protein or that the person is losing too much protein through urine or stool. Liver disease, kidney disease, or malnutrition, either from lack of protein in someone’s diet or from GI conditions that interfere with protein absorption, can lead to low albumin levels. Low pre-albumin levels are more specific to protein malnutrition.
Liver tests like aspartate transaminase (AST), alanine transaminase (ALT), and bilirubin (a product of breaking down red blood cells that causes jaundice at high levels in the blood) check how well the liver is working and for inflammation or damage. High AST and ALT levels show that there is damage to liver cells (hepatitis) from infection or autoimmunity. This damage can also be caused sometimes by medications and nutritional supplements. High bilirubin can happen if the liver is not making bile normally or if there is a blockage of the bile ducts themselves.
Other tests that a healthcare provider uses to diagnose digestive system problems include:
- Hydrogen breath test for SIBO.
- D-xylose absorption test, which checks how well the small intestines can absorb sugars by measuring d-xylose in your urine and blood after drinking it.
- Esophageal manometry, which measures the strength and coordination of the esophagus’ muscle contractions to understand symptoms of swallowing difficulties.
- 24-hour ambulatory pH monitoring to look for excess exposure of the esophagus to stomach acid that could cause damage (a condition known as reflux esophagitis).
General diarrhea and upset stomach care
Diarrhea means having stools (bowel movements) that are frequent, loose, and watery. It is a general GI symptom that can be caused by an infection (infectious diarrhea) or by inflammation unrelated to an infection. Some medications, including those used to treat GI infections, like antibiotics, can also cause diarrhea. Diarrhea can be mild or severe, depending on how often you go to the bathroom, and the amount and consistency of the stools.
Upset stomach (dyspepsia) is when you have upper abdominal discomfort, nausea, and vomiting or dry heaves. Like diarrhea, both GI infections and conditions that are not related to infections can cause an upset stomach.
If diarrhea is severe, it can cause dehydration, which means your body loses too much water. Babies, young children, and older adults are more likely to have serious problems from dehydration. Sometimes, GI infections cause both diarrhea and vomiting, which increases the dehydration risk. Signs of dehydration include:
- Skin that does not bounce back quickly when pinched.
- Dry lips, tongue, and mouth.
- Feeling unusually thirsty.
- Peeing less than usual.
- In babies, soft spots on the head (fontanelles) look sunken.
- Eyes that look sunken.
- Changes in behavior, like being restless or very tired and weak.
Supportive care for diarrhea includes replacing the fluids and salts your body has lost to prevent dehydration. If you have mild diarrhea, you can try changing your diet and drinking more fluids to make up for the loss. Your healthcare provider may suggest a clear liquid diet (avoiding milk products), including weak tea, sports drinks, broth, and flat soda without bubbles. As you start to feel better and your bowel movements become less frequent and smaller, you can slowly start eating more solid foods. If you are severely dehydrated from diarrhea, you may need to go to the hospital and get intravenous (IV) fluids.
Older children and adults should rinse their mouths with water often to help with mouth dryness and bad taste from being sick, especially after throwing up.
Sometimes, antibiotics themselves may cause diarrhea. The job of antibiotics is to kill bacteria. In some cases, they kill good bacteria that are part of your GI microbiome as well as the infection-causing ones. Your healthcare provider may recommend taking a probiotic when you are on antibiotics to replace some of the good bacteria. However, the benefit of probiotics is still controversial and, because they contain live bacteria and are not regulated by the FDA, they can pose a risk to PI patients. Only take probiotics as directed by your healthcare provider.
Sometimes the frequent bowel movements and repeated wiping with toilet paper that happens with diarrhea can lead to irritation of the skin around the anus. To feel more comfortable, you can coat the rectal area with petroleum jelly or other barrier creams used for diaper rash. This will protect the skin and reduce irritation from frequent bowel movements. Dirty diapers and clothes should be changed right away and anyone handling dirty diapers, clothes, or linens should immediately wash their hands.
This page contains general medical and/or legal information that cannot be applied safely to any individual case. Medical and/or legal knowledge and practice can change rapidly. Therefore, this page should not be used as a substitute for professional medical and/or legal advice. Additionally, links to other resources and websites are shared for informational purposes only and should not be considered an endorsement by the Immune Deficiency Foundation.
Adapted from the IDF Patient & Family Handbook for Primary Immunodeficiency Diseases, Sixth Edition.
Copyright ©2019 by Immune Deficiency Foundation, USA.
Sign up for updates
Receive news and helpful resources to your cell phone or inbox. You can change or cancel your subscription at any time.
