
-
Understanding primary immunodeficiency (PI)
Understanding PI
The more you understand about primary immunodeficiency (PI), the better you can manage it. Learn about PI diagnoses and treatment options.
-
Living with PI

Living with PI
Living with primary immunodeficiency (PI) can be challenging, but you’re not alone—many people with PI lead full and active lives. With the right support and resources, you can, too.
-
Get involved

Get involved
Be a hero for those with PI. Change lives by promoting primary immunodeficiency (PI) awareness and taking action in your community through advocacy, donating, volunteering, or fundraising.
-
Advancing research and clinical care

Advancing research and clinical care
Whether you’re a clinician, researcher, or an individual with primary immunodeficiency (PI), IDF has resources to help you advance the field. Get details on surveys, grants, and clinical trials.

Key points:
- Many people with or who are carriers of PI have had healthy pregnancies and deliveries.
- However, individuals with PI and carriers of PI may be at increased risk of fertility and pregnancy complications, including infections, bleeding (or, conversely, clotting), and flares of autoimmune or autoinflammatory symptoms. The risk of these complications depends on the type of PI involved.
- People with PI should discuss their reproductive health and family planning concerns early on with a multidisciplinary team of healthcare providers. This team may include geneticists, immunologists, hematologists, rheumatologists, obstetrician-gynecologists (OB/Gyn), maternal-fetal medicine (MFM) specialists, high risk OBs, and others.
- Clear communication with OB/Gyn providers about a PI diagnosis is important for closer monitoring throughout pregnancy, and close post-delivery monitoring of both mother and baby are essential.
- Immunoglobulin (Ig) replacement therapy is safe and essential for mothers with certain types of PI during pregnancy to provide antibodies that keep both mother and baby healthy.
- Some medications used to treat PI can affect fertility and pregnancy. The decision on how to adjust dosing or whether to discontinue these medications during pregnancy should be discussed carefully with your immunologist and OB/Gyn.
How PI affects pregnancy outcomes
There are few studies examining pregnancy outcomes in individuals with PI, which is why much more research needs to be done in this area. Most information on the ability of people with PI to become pregnant and their pregnancy outcomes comes from surveys of women diagnosed with common variable immune deficiency (CVID) and other antibody deficiencies. A few studies have included people with other types of PI, such as primary immune regulatory disorders (PIRDs) or autoinflammatory disorders. Because PI can take many years to be recognized, many women with PI symptoms may have completed childbearing before being diagnosed.
A 2015 survey of 490 women with self-reported CVID diagnoses and 100 women with self-reported hypogammaglobulinemia diagnoses found that [1]:
- About 75% of all respondents reported that they did not have difficulty getting pregnant.
- More than 70% of respondents who were already diagnosed at the time of their first pregnancy reported concerns about 1) their ability to have children, 2) their children being affected by the same PI, and/or 3) increased health risks during pregnancy.
- 50% of the respondents that had a PI diagnosis before they had children had reproductive health and family planning concerns, in comparison to 25% of undiagnosed and untreated women. The former also reported their PI diagnosis as having more impact on their decision to try for conception.
- Out of 966 pregnancies reported in the survey, 695 (72%) resulted in a live birth; in comparison, in 2008, 62% of pregnancies resulted in live births in the general U.S. population.
- The majority of the pregnancies reported did not have complications.
- Most people continued with immunoglobulin (Ig) replacement therapy during pregnancy.
- The rates of miscarriage reported by survey respondents for first and second pregnancies were similar to the U.S. national average.
- Fewer terminations of pregnancies were reported than the U.S. national average.
- At the time of the survey, 15% of children born to mothers with CVID were diagnosed with an antibody deficiency; 44% were diagnosed with CVID and 14% had selective IgA deficiency (SIgAD).
- Of those who had a child with a PI, 60% reported that this did not have an impact on their decision to have more children.
A study from the Czech National Registry of Reproduction Health on 54 women with CVID reported 115 total pregnancies, 88 (77%) of which resulted in live births [4]. This study found that miscarriages were more common in women who had PI symptoms while pregnant but were not yet diagnosed. However, pregnancy complications, such as low birth weight babies, high blood pressure (preeclampsia/eclampsia), and stillbirths, happened at similar rates regardless of whether the women had PI symptoms or were receiving treatment.
More recently, a study documented pregnancy outcomes in 93 women with PI living in France [5]. Twenty-seven of the women had a combined immunodeficiency (CID), 51 had an antibody deficiency, and 15 had innate immune disorders. Altogether, they had 222 pregnancies with 157 live births (71%). Four of the live births, or 3%, were severely premature. Overall, these outcomes were similar to the French general population. However, the study found that women with a history of severe infection were more likely to miscarry or terminate their pregnancy. Notably, only 59% of the pregnancies involved infection prevention appropriate for the pregnant person’s diagnosis, such as antibiotic/antifungal prophylaxis and/or Ig replacement therapy.
Familial Mediterranean fever (FMF) is the best studied autoinflammatory PI in terms of reproductive outcomes. Women with FMF have an increased risk of infertility or reduced fertility, as well as pregnancy loss, preterm labor, and stillbirth compared to the general population. However, the overall risk of stillbirth appears low, and fertility is usually preserved, although active or uncontrolled disease can reduce fertility in some women. Good disease control, especially with colchicine therapy, improves fertility and pregnancy outcomes and is considered safe during pregnancy and breastfeeding [6], [7,8]. Researchers have noted similar fertility and pregnancy complications with many other autoimmune or inflammatory conditions that someone with PI may also have, such as rheumatoid arthritis, systemic lupus erythematosus (SLE), celiac disease, thyroid autoimmunity, and endometriosis [9,10].
Unfortunately, for many other PIs, researchers have only published isolated case reports or case series.
Managing PI during pregnancy
Healthcare providers caring for a pregnant individual with PI have to carefully balance the need to treat the mother’s PI to reduce the risk of complications with the need to protect the developing baby.
Pregnant individuals with PI should receive all vaccines routinely recommended in pregnancy by the American College of Obstetricians and Gynecologists (ACOG) to protect themselves from infections and to support the baby’s growing immune system [15,16].
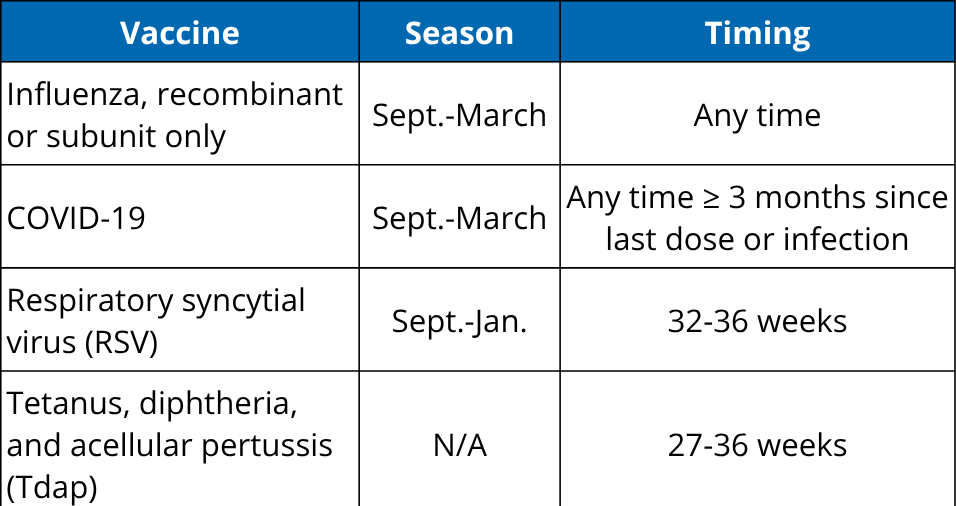
These immunizations are safe and recommended even in individuals on Ig replacement therapy or immunosuppressants. First, Ig products generally do not protect against current seasonal virus strains, such as the newest influenza or COVID-19 variants because of the time it takes to manufacture them. Second, patients with antibody deficiencies may still make T cell responses to vaccines that provide some protection against severe infection [17]. Finally, if the mother makes any IgG antibodies in response to vaccines, they will be transferred through the placenta to the baby. Since newborn babies cannot make their own antibodies (even if they don’t have PI) until they are 4-6 months of age, these transferred antibodies are an important layer of protection for them in early life.
Help your pregnancy care provider understand PI
Choose the template that fits your situation—one for individuals diagnosed with PI, and one for carriers of X‑linked PI (symptomatic or not). Both can be tailored with guidance from your immunologist to clearly communicate relevant risks, treatments, and your monitoring needs during pregnancy.

Newborns in families with PI
For the newborn baby of an individual with PI, there may be a number of concerns. These concerns include whether the baby has PI, as well as potential health effects from the birthing parent’s PI or medications taken during pregnancy. The newborn should be followed carefully by a pediatrician who knows about the parent’s PI. It may be helpful to have a provider on the parent’s healthcare team explain the condition and any risks to the baby to the pediatrician.
After delivery, most newborns in the U.S. receive newborn screening (NBS) for a number of severe genetic disorders. Severe combined immune deficiency (SCID) is one of these disorders, and the screening test for SCID also screens for other types of PI that lead to very low numbers of T cells, a type of white blood cell. However, it is important to keep in mind that NBS only screens for a very limited handful of PIs. It is also important to understand that newborn screening cannot diagnose SCID or any other PI. Abnormal screening results flag a baby for further testing to determine if they have SCID or not.
If the gene variant responsible for the parent’s PI has been identified (i.e., you have a genetic diagnosis), the baby can be tested for the variant after birth. Depending on which parent has PI and the sex of the child, they may be a carrier or may be at risk of developing the parent’s condition. As with all genetic testing, it’s important to have pre- and post-test genetic counseling to understand your testing options and what the possible outcomes could be.
If the child has inherited the PI-causing variant and could develop PI, then they should be seen by a pediatric clinical immunologist, rheumatologist, and/or geneticist, depending on the specific condition in question. These providers can diagnose the baby and run tests to understand the current state of the baby’s immune system. This baseline helps to determine whether the baby needs immediate treatment or ongoing monitoring.
If the parent with PI does not have a genetic diagnosis and the newborn is healthy, they can be followed by a general pediatrician and referred to the appropriate pediatric specialist if they develop PI symptoms.
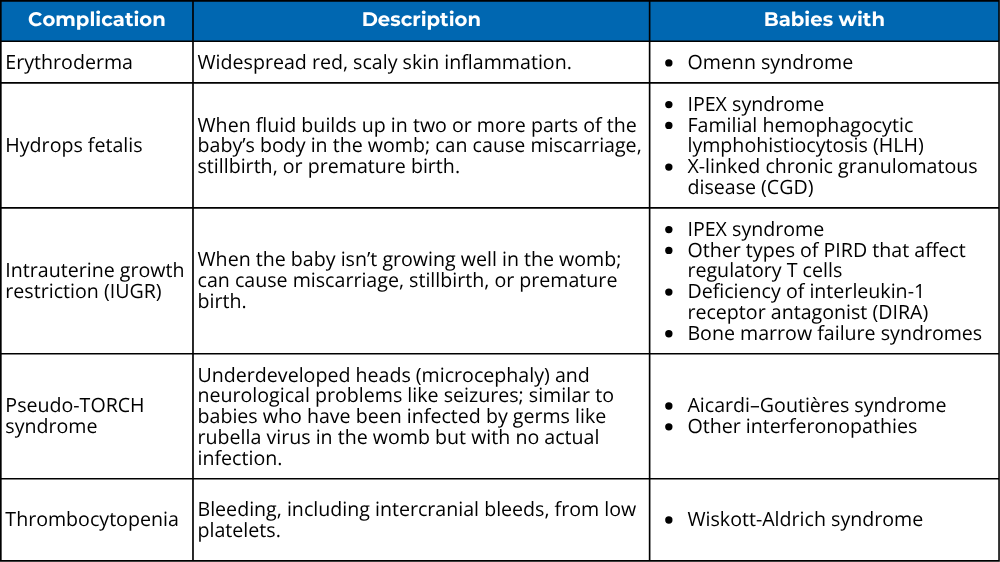
A recent review summarized some of the signs and symptoms that researchers have reported in babies with specific types of PI, either while still in the womb or as newborns [19]. In general, these very early signs are more common for PIs that have significant immune dysregulation symptoms.
For newborns of parents with antibody deficiencies, it may take longer for an immunodeficiency to reveal itself. Babies start to naturally make their own IgG when they are 4-6 months old, but they make their own IgA and IgM antibodies at birth since these are not transferred through the placenta in pregnancy. It may take several years, sometimes into early teenage years, to determine whether a child has inherited an antibody deficiency.
Finally, if the mother continues taking immunosuppressants or other medications aside from Ig during pregnancy, these may affect the baby’s development, including their immune system. However, these effects have not been well studied in most cases. If these medications have been continued through pregnancy, the newborn should be monitored for potential complications and have their immune system checked.
Related resources

Primary immunodeficiency in 2026: New practice parameters, genetic testing, and what's changed for patients
May 27, 2026
Listen to podcast

Kids Korner: How Ig infusions help people with PI stay healthy
May 20, 2026
Read article
Whole genome sequencing and the future of newborn screening
April 20, 2026
Watch video
This page contains general medical and/or legal information that cannot be applied safely to any individual case. Medical and/or legal knowledge and practice can change rapidly. Therefore, this page should not be used as a substitute for professional medical and/or legal advice. Additionally, links to other resources and websites are shared for informational purposes only and should not be considered an endorsement by the Immune Deficiency Foundation.
Adapted from the IDF Patient & Family Handbook for Primary Immunodeficiency Diseases, Sixth Edition.
Copyright ©2019 by Immune Deficiency Foundation, USA.
Sign up for updates
Receive news and helpful resources to your cell phone or inbox. You can change or cancel your subscription at any time.
