
-
Understanding primary immunodeficiency (PI)
Understanding PI
The more you understand about primary immunodeficiency (PI), the better you can live with the disease or support others in your life with PI. Learn more about PI, including the various diagnoses and treatment options.
-
Living with PI

Living with PI
Living with primary immunodeficiency (PI) can be challenging, but you’re not alone—many people with PI lead full and active lives. With the right support and resources, you can, too.
-
Get involved

Get involved
Be a hero for those with PI. Change lives by promoting primary immunodeficiency (PI) awareness and taking action in your community through advocacy, donating, volunteering, or fundraising.
-
Advancing research and clinical care

Advancing research and clinical care
Whether you’re a clinician, researcher, or an individual with primary immunodeficiency (PI), IDF has resources to help you advance the field. Get details on surveys, grants, and clinical trials.

Respiratory viruses can cause serious illness
- For some respiratory illnesses, particularly COVID-19 and RSV, primary immunodeficiency (PI), also known as inborn errors of immunity (IEI), is a risk factor for severe infections.
- Get emergency medical attention right away if you have:
- Trouble breathing.
- Lasting pain or pressure in your chest.
- Severe sore throat with fever.
- New-onset confusion.
- Inability to wake up or stay awake.
- Pale, gray, or blue-colored skin, lips, or nail beds, depending on skin tone.
- Vomiting or diarrhea leading to dehydration.
- A fever over 103°F.
How to avoid respiratory viruses
One of the most effective ways to avoid getting sick during respiratory virus season is to get vaccinated. However, you can’t get vaccinated against all respiratory viruses, so protecting yourself from exposure is also important.
Respiratory viruses mostly spread through the air when an infected person coughs, sneezes, talks, or exhales. Others then inhale or come in contact with tiny droplets that have viral particles. The viral particles enter the body through mucous membranes in the nose, mouth, and eyes. Strategies like boosting airflow and avoiding sick people help protect you against transmission through the air.
Respiratory viruses can also be spread by touching a surface contaminated with the virus and then touching your face. Washing your hands and limiting how much you touch your face protect you against transmission through surfaces.
Stay up to date with your shots
Unfortunately, you can’t get vaccinated against all respiratory viruses. However, there are vaccines against COVID-19, influenza, and RSV that provide good protection against the big three that cause the most serious infections.
For influenza and COVID-19, the World Health Organization (WHO) updates its recommendations for which strains vaccines should target every year, since these viruses change quickly. Because these vaccines change every year to match circulating virus strains, everyone 6 months of age or older needs flu and COVID-19 vaccines every year.
Why should everyone be immunized? First, many people with PI develop at least some antibodies or a T cell response (which is important for controlling viral infections) to the vaccines.
Second, although immunoglobulin (Ig) replacement therapy products (IVIG or SCIG) contain antibodies to flu and COVID, they typically do not have protective levels of antibodies against current virus strains because manufacturing takes 9-12 months after the initial plasma donation. For people on Ig, flu and COVID-19 vaccines can provide an extra layer of protection. Also, people on Ig replacement therapy do not need to coordinate vaccine timing with their treatment for these seasonal vaccines.
Finally, household members of people with PI should get vaccinated to create a "protective cocoon" around the person with PI. This strategy decreased the chances the person with PI will come in contact with the viruses.
The current 2025-2026 COVID-19 vaccines target the LP.8.1 strain and became available in September 2025. Because of their limited FDA approval and a recommendation for shared decision-making by the CDC, accessing the 2025-2026 COVID-19 vaccine differs by state. Talk to your healthcare provider and/or pharmacy to find out where you can get the shot.
The American Academy of Family Physicians (AAFP) and the American Academy of Pediatrics (AAP) recommend that the following groups receive at least one dose of the most current COVID-19 vaccine:
- Everyone aged 6-23 months old.
- People aged 2-18 years old who:
- Are at high risk of severe COVID-19, including those with PI.
- Reside in long-term care facilities or other group settings.
- Have never been vaccinated against COVID-19.
- Live with individuals that are at high risk of severe COVID-19, including those with PI.
- Everyone aged 19 years old or older.
- AAFP recommends that people 65+ years old get two doses at least two months apart.
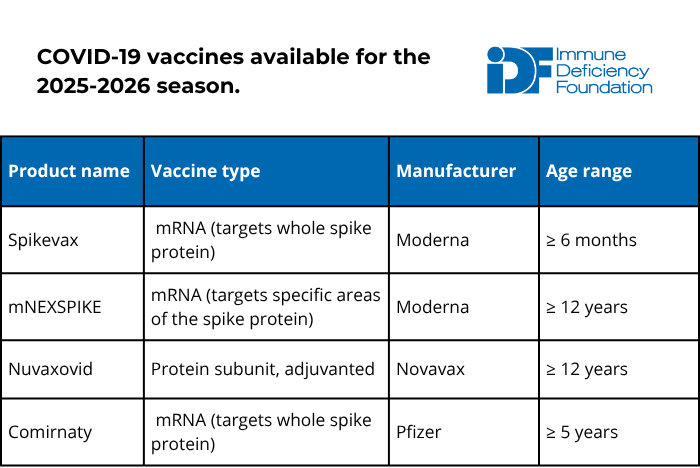
Discuss AAFP’s recommendations for those who are moderately to severely immunocompromised with your immunologist to determine whether you should receive more than one dose. In general, booster doses should be spaced out by at least two months.
The COVID-19 vaccine is safe and cannot cause COVID-19 in anyone, no matter how weak their immune system, because it does not contain live virus. Although there is no data in patients with PI, receiving the most recent COVID vaccine booster may prevent or reduce long COVID complications.
For the 2025-2026 season, all flu vaccines are trivalent, which means they protect against three different influenza virus strains: two influenza A strains and one influenza B strain.
There are multiple types of flu vaccines available and selecting the right type is important. The inactivated or recombinant flu vaccine types are best for people with PI and their household members. People with PI and their household members should not receive the live attenuated flu vaccine (trade name Flu Mist).
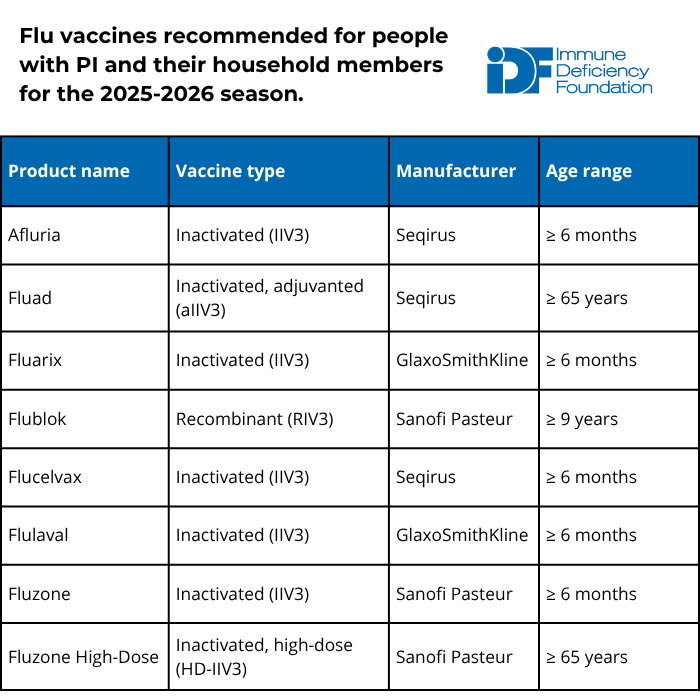
Additional recommendations from the American Academy of Pediatrics (AAP) and the American Academy of Family Physicians (AAFP) include:
- People aged 65+ should receive the high-dose inactivated, adjuvanted inactivated, or recombinant vaccine because these formulations provide greater protection in older individuals.
- Solid organ transplant recipients aged 18-64 who are on immunosuppressants can also receive either high-dose inactivated or adjuvanted inactivated influenza vaccines.
- Children 8 years old or younger who have not received at least two flu vaccine doses previously should receive two doses of flu vaccine spaced four weeks apart.
- People with egg allergy may receive any vaccine (egg-based or non-egg-based) that is appropriate for their age and health status.
The flu vaccine is safe, and the inactivated and recombinant versions cannot cause the flu in anyone, no matter how weak their immune system. The vaccine is available from late summer, and AAP and AAFP recommend getting vaccinated by mid-October for the best protection through flu season.
The U.S. Food and Drug Administration (FDA) has approved five preventative products for RSV within the last couple of years: three vaccines and two long-lasting monoclonal antibodies. Unlike vaccines, monoclonal antibodies are a type of passive immunization that provide protection regardless of how well a person’s immune system works. Monoclonal antibodies work like immunoglobulin replacement therapy but only protect against one specific germ.
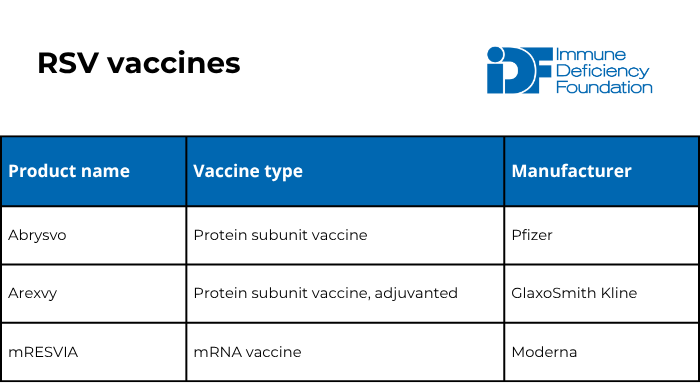
The American Academy of Family Physicians (AAFP) recommends that the following people get an RSV vaccine:
- Pregnant individuals who have not received an RSV vaccine previously. These individuals should get one dose of the Abrysvo vaccine when they are 32-36 weeks pregnant from September through January.
- People aged 50-74 who are at high risk of severe RSV infection (including those who are moderately or severely immunocompromised).
- People age 75+.
Unlike the flu and COVID-19, experts consider RSV vaccination protective for a long period of time. There are currently no recommendations for any group to receive more than one dose in their lifetime.
The RSV vaccine is safe and cannot cause RSV in anyone, no matter how weak their immune system, because it does not contain live virus.
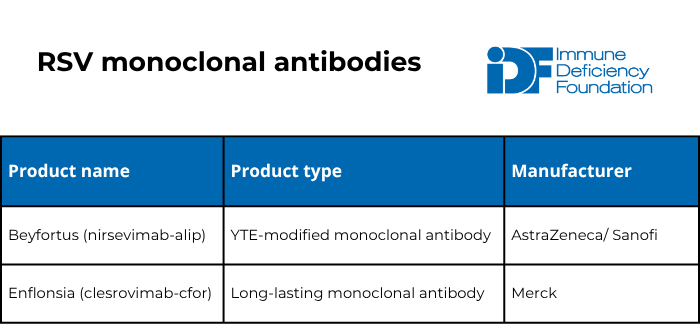
The American Academy of Pediatrics (AAP) recommends one dose of either of the two long-lasting monoclonal antibodies for:
- Babies 7 months old or younger born to individuals who have never been vaccinated for RSV or were vaccinated for RSV during a previous pregnancy.
- Babies 8-19 months old who are at high risk of severe RSV infection either because of a medical condition (including severe immunocompromise) or because of American Indian/Native Alaskan heritage.
Consider getting the anti-COVID-19 monoclonal antibody
The FDA approved pemivibart, made by Invivyd (trade name Pemgarda), in March 2024. Pemgarda is a monoclonal antibody, which means that unlike vaccines, it provides protection regardless of how well a person’s immune system works. It is meant to be used before exposure to prevent COVID-19 infections in those who are at least 12 years of age, weigh at least 88 pounds, and are moderately to severely immunocompromised. It is not approved for use after exposure or during infection.
Pemgarda is an intravenous infusion given every three months and must be prescribed by a healthcare provider. Infectious Disease Society of America’s clinical guidelines for Pemgarda can help healthcare providers determine if their patients should receive it. It is typically given at an infusion center or other healthcare facility and any facility can order it through their distributor; see Invivyd’s facility locator for help finding a location.
Stop the spread
While vaccines are a crucial tool during respiratory virus season, you should take advantage of other tools, too:
- Regularly wash your hands with soap and water for 20 seconds, especially after coughing or sneezing. If soap and water aren’t available, use hand sanitizer with at least 60% isopropanol or 70% ethanol. Note that hand sanitizer may not be as effective in killing germs as handwashing.
- Keep away from individuals who are sick.
- Disinfect high-touch surfaces in your home, like door handles and light switches.
- Try not to touch your nose, mouth, or eyes.
- In crowded indoor areas, use a well-fitted N-95 or KN-95 mask covering your nose and mouth to avoid inhaling droplets that can spread respiratory viruses.
- During respiratory virus season, those with PI should consider avoiding crowded indoor areas such as shopping malls.
- When coughing or sneezing, cover your nose and mouth with a sleeve, elbow, or tissue. Dispose of the tissue after use.
- Stay home from work or school while sick and consider masking around others for up to five days after feeling better.
Boost indoor airflow
Respiratory viruses spread through the air, so crowded, indoor spaces with poor airflow increase the possibility of a sick person infecting others. Simple actions you can take include:
- Opening windows and doors.
- Setting HVAC system fans to run continuously.
- Using high-filtration HVAC filters and replacing them often.
- Using air purifiers/cleaners that meet certain criteria.
Latest infectious disease resources

Foundation to follow medical societies' vaccine schedules in light of ACIP hepatitis B decision
December 09, 2025
Read statement

Preparedness key when visiting emergency department with PI
September 30, 2025
Read article

Update: ACIP meeting adds to COVID-19 vaccine confusion
September 24, 2025
Read article
This page contains general medical and/or legal information that cannot be applied safely to any individual case. Medical and/or legal knowledge and practice can change rapidly. Therefore, this page should not be used as a substitute for professional medical and/or legal advice. Additionally, links to other resources and websites are shared for informational purposes only and should not be considered an endorsement by the Immune Deficiency Foundation.
Sign up for updates from IDF
Receive news and helpful resources to your cell phone or inbox. You can change or cancel your subscription at any time.