
-
Understanding primary immunodeficiency (PI)
Understanding PI
The more you understand about primary immunodeficiency (PI), the better you can manage it. Learn about PI diagnoses and treatment options.
-
Living with PI

Living with PI
Living with primary immunodeficiency (PI) can be challenging, but you’re not alone—many people with PI lead full and active lives. With the right support and resources, you can, too.
-
Get involved

Get involved
Be a hero for those with PI. Change lives by promoting primary immunodeficiency (PI) awareness and taking action in your community through advocacy, donating, volunteering, or fundraising.
-
Advancing research and clinical care

Advancing research and clinical care
Whether you’re a clinician, researcher, or an individual with primary immunodeficiency (PI), IDF has resources to help you advance the field. Get details on surveys, grants, and clinical trials.

Key points
- The immune system touches many different parts of the body. Oftentimes, the first symptoms of primary immunodeficiency (PI) show up as infections, autoimmunity, or inflammation in one or more body systems.
- Healthcare providers should test the immune system of anyone who develops unusual, severe, or multiple infections and/or inflammatory or autoimmune conditions to see if they have an undiagnosed PI.
- Meningitis, encephalitis, and sepsis are conditions that people with many types of PI can develop that are medical emergencies.
- To check for eye problems, people with PI should get yearly eye exams by an eye specialist (ophthalmologist).
- Sometimes, to treat inflammatory or autoimmune conditions in other organ systems, specialists may have to use immunosuppressants in a person with PI. Specialists should always work with the person’s immunologist to balance treating the condition with preventing infections.
Because you need a working immune response to prevent and clear infections, people with primary immunodeficiency (PI) often have more frequent or severe infections than people without PI. In addition, people with many kinds of PI can develop conditions caused by an imbalance in the immune system known as immune dysregulation. One type of immune dysregulation is autoimmunity, where either T cells (autoreactive T cells) or antibodies from B cells (autoantibodies) target healthy tissue. Another type is chronic inflammation, where the immune system is generally overactive and healthy tissue becomes collateral damage.
Any organ or part of the body can be infected by germs, become the target of autoimmunity, or be damaged by chronic inflammation in someone with PI. Note that respiratory and digestive system symptoms are common across many types of PI, so they have their own pages. This page addresses the infections and autoimmune/inflammatory conditions most often seen in other body systems.
Always tell your healthcare provider as soon as possible if you develop new symptoms that could be caused by an infection, autoimmunity, or chronic inflammation. All three can lead to serious, permanent organ damage if they are not treated. Some conditions, especially certain infections, can quickly become life threatening. It is important to see a healthcare provider that understands that people with PI sometimes do not have typical responses to infections. For example, those with PI may not spike a fever or have high white blood cell counts even if they have a severe and life-threatening infection [1].
Depending on your symptoms, your immunologist may need to work with other specialists to properly diagnose and treat your condition.
Nervous system
In people with many types of PI, serious infections like meningitis and encephalitis can develop within the nervous system. In addition, specific PIs, such as ataxia-telangiectasia (A-T) and many combined immunodeficiencies (CIDs), have neurological symptoms that are part of the overall condition. These can include difficulty walking straight (ataxia), cognitive impairments, attention-deficit hyperactivity disorder (ADHD), autism spectrum disorder (ASD), seizures, or inflammatory lesions in the brain, and are covered in the chapters specific to those PIs [2].
Meningitis
Meningitis is inflammation of the lining of the brain and spinal cord (meninges). It is a serious and potentially life-threatening condition usually caused by bacterial, viral, or fungal infections. Note that drug-induced aseptic meningitis (DIAM), which sometimes happens as a side effect of intravenous immunoglobulin (IVIG) replacement therapy, is inflammation of the meninges that is not caused by an infection [3]. While DIAM is a serious IVIG side effect, it is not usually life-threatening and goes away on its own as few days after the infusion.
Symptoms of infectious meningitis include fever, severe headache, stiff neck, nausea or vomiting, and sensitivity to light (note that people with PI may not spike a fever in some cases). Meningitis is a medical emergency and people with these symptoms need to go to the emergency room right away. Emergency room providers will perform a physical exam and spinal tap (lumbar puncture) to test spinal fluid for the type of meningitis and the type of germ that may be causing it.
People with many different PIs are at risk of developing meningitis, but people with terminal complement deficiencies (C5-C9) or properdin deficiency are at particular risk for developing meningitis from Neisseria meningitidis bacteria [4]. This type of bacterial meningitis is especially dangerous.
Encephalitis
Encephalitis is inflammation of the brain itself. It can be caused by bacteria, fungi, or viruses (such as West Nile virus). It can also be caused by autoimmunity (autoimmune encephalitis). Symptoms include severe headache, confusion or altered mental state, fatigue, seizures, and a decrease in consciousness. Like meningitis, encephalitis is a medical emergency and people with these symptoms need to go to the emergency room right away.
To diagnose encephalitis, healthcare providers do blood tests such as a complete blood count (CBC), infectious studies such as spinal tap, magnetic resonance imaging (MRI), and neurologic examination. If an infection is causing the encephalitis, treatment includes treating the infection with antimicrobials. Treatment for both infectious and autoimmune encephalitis includes treating the inflammation with medications such as corticosteroids.
Blood
Sepsis
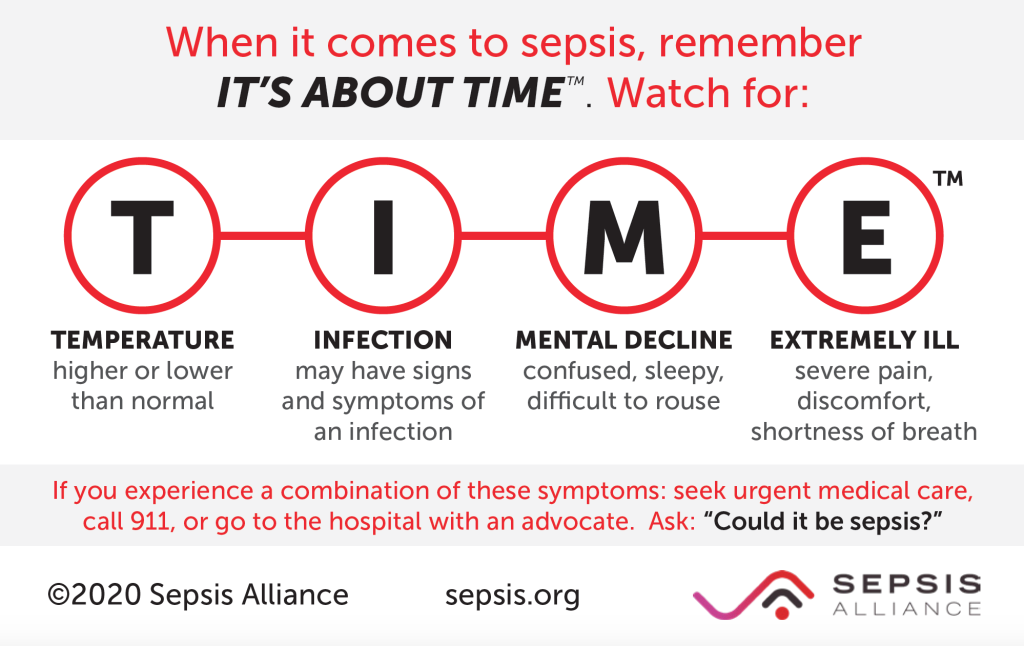
Many different kinds of germs like bacteria, viruses, and fungi can cause a serious condition called sepsis, which is an extreme, whole-body response to an infection. Another, older term for sepsis is blood poisoning and it is still sometimes referred to as a blood infection. However, sepsis is not an infection, it is the body’s response to an infection. It is an extremely serious and life-threatening condition. Like meningitis and encephalitis, sepsis is a medical emergency that needs to be diagnosed and treated immediately.
Signs of sepsis include a high fever or chills, mental confusion or extreme sleepiness, disrupted vital signs like low blood pressure and high heart rate, and, in some cases, severe pain or discomfort (note that people with PI may not spike a fever in some cases) [5]. It can develop gradually or suddenly. Young children may refuse to eat and have low urine output. Septic shock refers to late-stage sepsis that includes very low blood pressure.
To treat sepsis, healthcare providers have to draw blood cultures to figure out what kind of germ is causing the underlying infection. Very often, the infection needs to be treated with intravenous (IV) antimicrobials even before an exact germ can be identified.
Autoimmune cytopenias
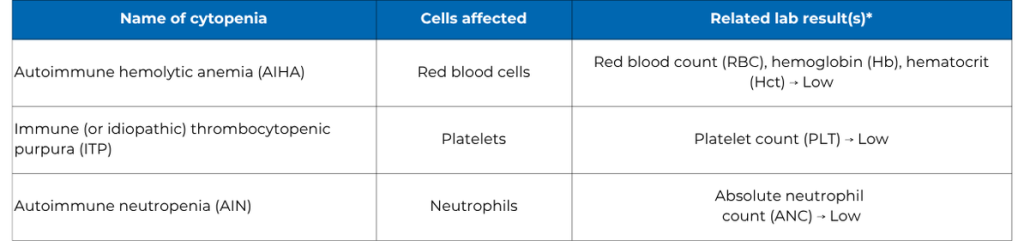
One of the most common types of autoimmunity seen across many types of PI is the development of autoantibodies that bind to and destroy healthy blood cells [6]. The blood cells affected can include red blood cells (RBCs), platelets, and white blood cells (WBCs). When autoantibodies destroy healthy blood cells, this leads to cytopenia, which is the general term for low numbers of blood cells.
Trauma or damage to body tissues can cause bleeding. Platelets, which are small cell fragments, help form blood clots to stop the bleeding. A low number of platelets is called thrombocytopenia. When the body makes autoantibodies that attack platelets, causing thrombocytopenia, it is called immune (or idiopathic) thrombocytopenic purpura (ITP).

ITP can lead to severe or prolonged bleeding. People with ITP often notice more bruising than usual, sometimes in unusual places or without a known injury. They might have a pinpoint red rash called petechiae, which is caused by small bleeds under the skin. They may have nosebleeds that happen more often, last longer, and are hard to stop. Their gums may bleed easily. Their urine might be pink or red. Their stool may look black and sticky, like tar, which can mean there is bleeding in the digestive system. In rare cases, bleeding in the brain can cause confusion or even death.
Diagnosing autoimmune cytopenias
Healthcare providers diagnose autoimmune cytopenias with blood tests. Usually, a complete blood count (CBC) with differential will show if someone has low numbers of red blood cells, different types of white blood cells, and/or platelets in their bloodstream.
To find out if the cytopenia is caused by autoimmunity, additional blood tests check for autoantibodies, although these antibodies are often difficult to detect. A specialist such as a clinical immunologist, hematologist, or oncologist typically evaluates individuals for these disorders. Sometimes, healthcare providers will do a bone marrow biopsy, which involves taking a sample of bone marrow tissue from the hip bone using a needle, to see if there is a problem with how the blood cells are made.
Treating autoimmune cytopenias
Autoimmune cytopenias may be temporary and if they get better on their own, they may not need much treatment. If they need to be treated, the goal is to get rid of the autoantibodies and allow the body to make more of the affected blood cell(s). The best treatment for a particular person depends on many factors and the particular type of cytopenia.
Treatment may include intravenous immunoglobulin (IVIG) therapy, corticosteroids, or other medications that suppress the immune system (immunosuppressants). Note that healthcare providers typically prescribe a higher dose of Ig to treat autoimmune cytopenias than to treat PI, so subcutaneous administration (i.e., SCIG) may not be an option.
In the past, healthcare providers regularly removed the spleen (splenectomy) in people with ITP. However, with newer therapies available, splenectomies are no longer the first line of therapy. In addition, since the spleen is an immune system organ, removing it increases the risk of severe infection in someone with PI, and should only be done with caution.
Autoimmune cytopenias often respond well to treatment. However, sometimes symptoms come back or need long-term treatment. People with autoimmune cytopenias rarely need blood transfusions unless their cytopenia is severe. In all cases, people with cytopenias need to be monitored regularly by their healthcare providers.
Most people with autoimmune cytopenias don't have to change their daily activities. However, people with low platelet counts may need to avoid activities with a higher chance of injury, like contact sports.
Kidneys
The kidneys are part of the urinary system and have many tiny filters called glomeruli. The kidneys remove a waste chemical called urea from the blood. Urea is the main chemical in urine. The kidneys also control water levels in the body and levels of chemicals like sodium and potassium (electrolytes).
Glomerulonephritis is inflammation of the glomeruli, which can permanently damage them. When the glomeruli are damaged, the kidneys can’t filter the blood as well and urea, a waste chemical, builds up in the bloodstream. Kidney function gets worse over time if the inflammation is not treated. People with very low kidney function may need dialysis, which is regular filtering of the blood by a machine, or a kidney transplant.
Sometimes, especially in children, glomerulonephritis is caused by the immune system’s reaction to an infection like strep throat (post-infectious glomerulonephritis). However, it can also be caused by autoimmunity or chronic inflammation.
Autoimmune or inflammatory glomerulonephritis is the most common chronic kidney condition in people with PI. People with complement deficiencies, especially in components C1-C4, often develop autoimmune glomerulonephritis [10]. Autoimmune glomerulonephritis can also happen, but not as often, in other PIs like IPEX syndrome and STAT3 gain of function (GOF). People with Wiskott-Aldrich syndrome (WAS) can develop glomerulonephritis caused by a kidney disease called IgA nephropathy [11]. In IgA nephropathy, immunoglobulin A (IgA) builds up in the kidneys.
Diagnosing glomerulonephritis
Often, the first sign of glomerulonephritis is high blood pressure (hypertension). The person may have blood or protein in their urine, which can cause the urine to look brownish, like tea or cola, or foamy. If the person is losing a lot of protein in their urine, they may have swelling in their legs and feet from their body retaining extra water (edema).
Common blood and urine tests can help determine how well someone’s kidneys are working. The urine tests look for blood, protein, and white blood cells and measure electrolyte levels. If your kidneys are not working well, your healthcare provider will refer you to a specialist called a nephrologist for diagnosis and treatment.
The nephrologist may do a kidney biopsy to make the correct diagnosis. A kidney biopsy is usually done by inserting a needle through the skin and into the kidney to get a small piece of tissue. This tissue is then examined by a specialist called a pathologist, who performs tests on it, including looking at it under a microscope.
Treating glomerulonephritis
Typically, post-infectious glomerulonephritis does not require treatment with antibiotics since the infection may have already cleared. If the infection is still present, your healthcare provider may prescribe antibiotics. Your healthcare provider may also prescribe blood pressure medications to manage any hypertension.
To manage autoimmune glomerulonephritis, nephrologists often use medications that suppress the immune system (immunosuppressants). Because immunosuppressants weaken a person’s immune system further, they can make people with PI even more likely to get infections. To balance treating autoimmune glomerulonephritis with preventing infections, your immunologist and nephrologist need to coordinate these treatments together.
Latest related conditions resources

Rheumatologist to discuss autoimmunity at National Conference
May 07, 2026
Read article

Neurologist to speak on brain and immune system at National Conference
March 24, 2026
Read article

Why PI affects the skin: Common rashes, infections, and immune dysregulation (dermatology deep dive)
February 03, 2026
Listen to podcast
This page contains general medical and/or legal information that cannot be applied safely to any individual case. Medical and/or legal knowledge and practice can change rapidly. Therefore, this page should not be used as a substitute for professional medical and/or legal advice. Additionally, links to other resources and websites are shared for informational purposes only and should not be considered an endorsement by the Immune Deficiency Foundation.
Adapted from the IDF Patient & Family Handbook for Primary Immunodeficiency Diseases, Sixth Edition.
Copyright ©2019 by Immune Deficiency Foundation, USA
Sign up for updates
Receive news and helpful resources to your cell phone or inbox. You can change or cancel your subscription at any time.
