
-
Understanding primary immunodeficiency (PI)
Understanding PI
The more you understand about primary immunodeficiency (PI), the better you can manage it. Learn about PI diagnoses and treatment options.
-
Living with PI

Living with PI
Living with primary immunodeficiency (PI) can be challenging, but you’re not alone—many people with PI lead full and active lives. With the right support and resources, you can, too.
-
Get involved

Get involved
Be a hero for those with PI. Change lives by promoting primary immunodeficiency (PI) awareness and taking action in your community through advocacy, donating, volunteering, or fundraising.
-
Advancing research and clinical care

Advancing research and clinical care
Whether you’re a clinician, researcher, or an individual with primary immunodeficiency (PI), IDF has resources to help you advance the field. Get details on surveys, grants, and clinical trials.

Key points:
- People with PI have a higher risk of severe respiratory tract infections such as pneumonia.
- In certain PIs, chronic inflammation of the lung not due to infection (non-infectious lung disease) can lead to permanent lung damage (fibrosis) if it is not diagnosed early and treated.
- Both respiratory infections and non-infectious lung disease can cause lung damage that gets worse over time, so it’s important to tell your healthcare provider about any breathing problems or other signs of lung disease so you can get properly diagnosed and treated.
- Vaccination against germs that cause respiratory infections, like influenza and COVID-19, helps prevent severe infections in many types of PI.
- The early diagnosis and treatment of influenza and COVID-19 can prevent severe infections, hospitalizations, and death.
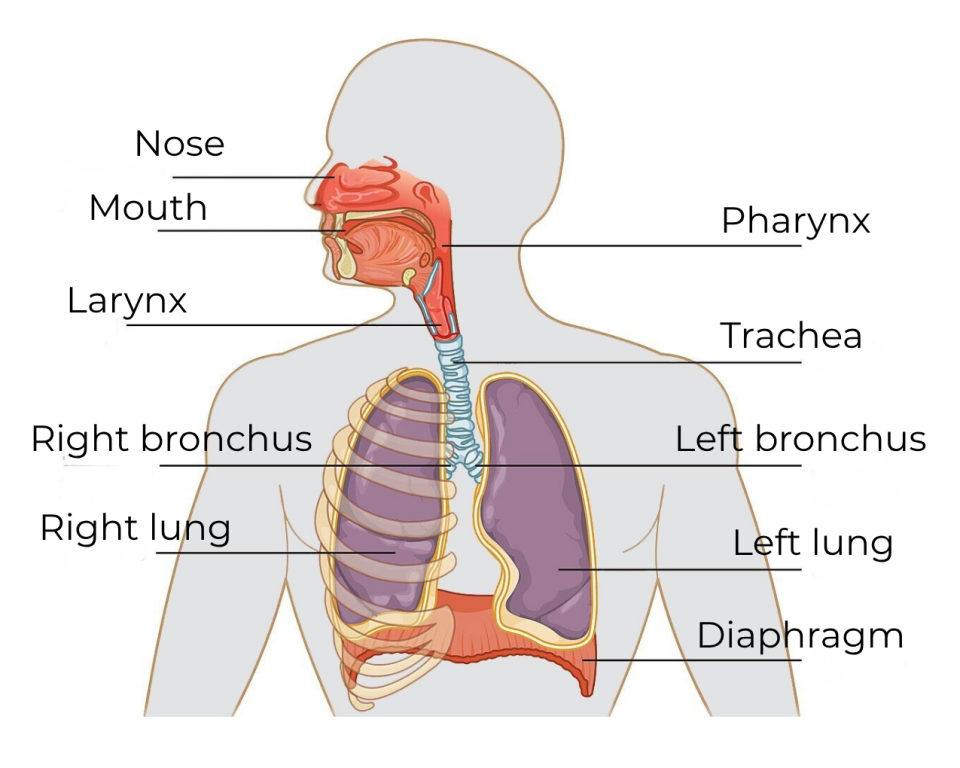
The respiratory system, or respiratory tract, refers to all the passageways and organs involved in breathing. The upper respiratory tract includes the mouth, nose, throat (pharynx), sinuses, and the upper part of the voice box (larynx). The lower respiratory tract includes the lower part of the voice box, the windpipe (trachea), the breathing tubes leading from the trachea to the lungs (bronchi and bronchioles), and the lungs themselves.
Your immune system works to prevent or clear an infection caused by germs such as bacteria or viruses. Inflammation is one way the immune response clears these infections. For example, when you get a cold, your immune response brings white blood cells and immune system proteins to the site of infection. When the infection is cleared, the extra white blood cells and inflammatory proteins go back to normal levels. Because you need a working immune response to prevent and clear infections, people with PI often have more respiratory tract infections and more severe respiratory tract infections than people without PI. These repeated infections can cause permanent damage to the airways.
Some lung disease caused by PI is not due to germs or the result of damage from infections (non-infectious lung disease). Instead, it is caused by an imbalance in the immune system known as immune dysregulation. One type of immune dysregulation is autoimmunity, where either T cells (autoreactive T cells) or antibodies from B cells (autoantibodies) target healthy tissue. Another type is chronic inflammation, where the immune system is not properly controlled. If it’s not treated, non-infectious lung disease gets worse over time and can cause scarring (fibrosis) that permanently reduces how well your lungs work.
Always let your healthcare provider know if you have symptoms of a respiratory infection or are having trouble breathing or catching your breath. Your provider may need to work with a lung specialist, called a pulmonologist, to properly diagnose and treat any lung conditions.
Respiratory tract conditions
Rhinitis
Rhinitis is inflammation of the mucous membranes in your nose. Common symptoms of rhinitis are runny nose (rhinorrhea), sneezing, cough, and congestion. Rhinitis can be acute (< four weeks) or chronic. The common cold is a frequent cause of acute rhinitis and usually gets better much sooner than four weeks.
On the other hand, chronic rhinitis has several different causes such as allergies, medications, irritants, chronic sinusitis, or structural problems in the nose. In addition to the symptoms of acute rhinitis, people with chronic rhinitis may have a decrease or loss of smell. If your rhinitis symptoms last longer than four weeks, you should see your healthcare provider to identify the cause of the problem.
Common cold
The common cold, also called coryza or an upper respiratory infection, is when the upper part of your respiratory tract (nose and throat) is inflamed because of a viral infection. Early signs are a scratchy or sore feeling in your throat, then sneezing, coughing, and a runny nose. You might also feel tired and have body aches.
There are many different viruses that can cause a cold but the most common is rhinovirus [1]. While testing for rhinovirus is available through healthcare providers, testing isn’t usually necessary unless the infection is severe. Over-the-counter medications can help you feel better, but there are no antiviral medications for rhinovirus or other cold-causing viruses. Antibiotics do not work for a cold because they kill bacteria, not viruses.
For people with most types of PI, a cold usually lasts about a week and will get better on its own. For people with untreated severe combined immune deficiency (SCID) or another PI that causes low T cells, a cold can become severe and needs immediate medical attention. If a cold lasts longer than a week and you have a fever, are coughing up mucus, or have trouble breathing, it could be something more serious, and you should see your healthcare provider.
Sinusitis
Sinusitis is inflammation of the mucous membranes lining your sinuses, which are small spaces in the facial bones around your nasal passages. Because mucous membranes in the nose can also be involved, healthcare providers sometimes use the term rhinosinusitis.
Your sinuses warm, humidify, and filter air before it goes into your lungs, help to reduce the weight of your skull, and affect the sound of your voice. The mucous membrane lining clears the sinuses by using tiny, hair-like structures called cilia to sweep mucus, particles, allergens, and germs out of the sinus cavities.
Pharyngitis and tonsillitis
Pharyngitis describes inflammation of the throat (sore throat). Tonsillitis is when the tonsils, which are located at the back of the throat, become inflamed. Symptoms include a raw or tickling sensation in the back of the throat and, sometimes, difficulty swallowing. Sometimes these symptoms are accompanied by a fever.
The majority of sore throats and tonsillitis are caused by viruses. Aside from influenza and COVID-19, there are no antiviral medications for viruses that cause a sore throat or tonsillitis. Antibiotics will not help for a viral infection.
However, sore throats that are caused by the bacteria Streptococcus pyogenes (strep throat) can cause rheumatic fever or kidney inflammation if they are not treated. If a person with PI has a sore throat, they should contact their healthcare provider to get a strep quick test or culture. Strep throat is usually treated with antibiotics and healthcare providers recommend throwing out toothbrushes and sanitizing water bottles or other objects that could harbor strep bacteria to keep from re-infecting yourself [5].
Sometimes, people have recurrent tonsillitis. In that situation, healthcare providers might suggest removing the tonsils. In children, providers may also recommend removing the adenoids, which are glands at the back of the upper airway, if they are also chronically inflamed. Adults typically do not have any adenoidal tissue or only a very tiny amount because the adenoids shrink in late childhood and adolescence.
Acute bronchitis
Acute bronchitis is inflammation of the bronchi, which are the tubes that carry air from your windpipe into your lungs. Usually, a respiratory virus or, much less commonly, bacteria cause acute bronchitis [6]. Frequently, acute bronchitis happens after a cold or other upper respiratory tract infection.
The most common symptom is a cough that usually lasts 1-3 weeks. The cough may bring up uncolored or colored mucus from the lower airways (sputum). A low-grade fever may occur in some cases of acute bronchitis. If you have a cough, high fever, or increasing shortness of breath, see your healthcare provider as soon as possible because the infection may involve your lungs (pneumonia). Antibiotics are not usually used for acute bronchitis and treatment focuses on controlling symptoms.
Croup
Croup is a general term for an infection, usually in children, that causes inflammation of the voice box (larynx), windpipe (trachea), and airways leading into the lungs (bronchi). Children ages 6 months to 3 years of age are at the highest risk for croup and it is uncommon past 6 years of age. Croup is most commonly caused by parainfluenza viruses, but other viruses can cause croup as well [7]. Bacteria are an uncommon cause of croup.
Croup can start suddenly or slowly. The child might have a normal or slightly high temperature. Sometimes, croup starts at night, and the child might wake up with a tight, barking cough (described as sounding like a seal barking) and trouble breathing. Breathing is hard because the windpipe narrows from inflammation.
Croup can be scary for both caregivers and kids. It’s important for caregivers to stay calm and reassure the child because their breathing can get worse if they become anxious. Home remedies that can help include sitting in a steamy bathroom or, conversely, breathing in cold air, either from outside or by standing in front of an open freezer [8].
If the child’s breathing gets worse, they may need quick medical help. Depending on how bad the symptoms are, caregivers should contact their healthcare provider or go to the emergency room.
Influenza
The flu is a term often used to describe the fever, body aches, cough, and congestion caused by many common respiratory viruses. However, only the influenza virus truly causes the flu.
The flu can be a very serious infection. For example, there were 28,000 flu-related deaths in the U.S. during the 2023-2024 flu season, and most adults hospitalized for the flu had a high-risk underlying medical condition [9], [10]. For most people with PI, the increased risk from the flu comes from complications like chronic lung disease. However, some rare PIs like IRF7 deficiency make a person very high risk for severe flu infections.
Fall and winter are typically flu season in the U.S. Flu symptoms include a sudden high fever, chills, headache, muscle aches, weakness, tiredness, and a runny nose. Vomiting and diarrhea can also occur. Sometimes, a bacterial infection of the ears (otitis media), sinuses (sinusitis), or even lungs (pneumonia) can develop during or after the flu.
You should speak with your healthcare provider right away if you think you have the flu or have been exposed to the flu. If you feel sick, immediately test with an unexpired, rapid antigen test at home. There are now a number of rapid antigen influenza A and B tests, as well as “multiplex” rapid antigen tests that test for COVID-19, influenza A, and influenza B all at the same time.
There are four antiviral drugs available to treat the flu, but they need to be started 1-2 days after symptoms begin to be most effective. All four work on both influenza A and influenza B viruses. If used early, they decrease severe flu infections, hospitalizations, and deaths in people at risk for severe flu (like people with PI). Three of these antiviral medicines can also be used to prevent getting the flu if you are exposed to someone who has the flu.
The best way to prevent the flu is to keep up to date with yearly influenza vaccinations. People with PI and their caregivers should not be immunized with the live, attenuated influenza vaccine (Flu Mist) but should receive one of the inactivated or recombinant flu vaccines every year. Even those on Ig replacement therapy should get a flu vaccine because Ig products typically do not have enough protective antibodies to current flu strains.
COVID-19
People with PI should discuss plans with their healthcare provider for dealing with COVID-19, including:
- How and where will you get tested for COVID-19 or other, similar respiratory viruses like influenza?
- What antiviral medication(s) does your healthcare provider recommend and how will you get them?
- Does your healthcare provider recommend receiving convalescent plasma? If so, where will you get it? Note that only hospital-based providers can order this product.
COVID-19 is a contagious respiratory disease caused by the coronavirus SARS-CoV-2. The SARS-CoV-2 virus spreads mainly through the air when an infected person coughs, sneezes, talks, or exhales [11]. Others then inhale or come in contact with viral particles. The viral particles enter the body through mucous membranes in the nose, mouth, and eyes. Less commonly, COVID-19 can also be spread by touching contaminated surfaces and then touching your nose, mouth, or eyes.
Symptoms of COVID-19 vary from person to person, with some people experiencing no or mild symptoms while others experience life-threatening disease. COVID-19 symptoms can include fever or chills, cough, fatigue, muscle or body aches, headache, new loss of taste or smell, sore throat, stuffy or runny nose, nausea or vomiting, diarrhea, and shortness of breath. At the onset of COVID-19, people may have mild symptoms similar to a cold. However, mild symptoms at the beginning of the infection do not mean you will not develop severe disease later on.
Most commonly, COVID-19 causes respiratory tract infections, and severe pneumonia is a common cause for hospitalizations and death. However, COVID-19 can also affect other parts of the body including the heart, blood vessels, kidneys, and other organs.
People with PI are at higher risk for severe COVID-19 and death than the general population [12]. A study looking at the entire population in Sweden found that people with PI were 3-4 times more likely to be hospitalized and five times more likely to be admitted to the intensive care unit than those without PI [13]. People with PI were also more likely to die from COVID-19.
Other risk factors for severe COVID-19 infections are common to people in the general population and to those with PI. These include, but are not limited to:
- Being 65+ years old.
- Having chronic lung, liver, kidney, or heart disease, or cancer.
- Being on medication that suppresses the immune system.
While all types of PI increase someone’s risk of developing severe COVID-19, there are specific PIs that put individuals at very high risk. Type I interferons are immune system proteins that help fight viral infections and are especially important in preventing severe COVID-19 infections. PIs that disrupt the type I interferon response like TLR7 deficiency place people at very high risk of developing severe COVID-19. In autoimmune polyendocrinopathy syndrome type 1 (APS-1, also known as autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy or APECED), the immune system makes antibodies against type I interferons, so people with APS-1/APECED are also a very high risk of severe COVID-19 infections [14].
If you have symptoms of a respiratory tract infection, immediately test for COVID-19 using an unexpired, rapid antigen test at home. Keep in mind that rapid antigen tests may be negative early in an infection even if you really do have COVID-19. If the rapid test is negative, consider getting a more sensitive PCR test (sometimes called a NAAT test) and testing for other respiratory viruses. These tests are typically available at pharmacies, urgent care centers, and healthcare provider offices.
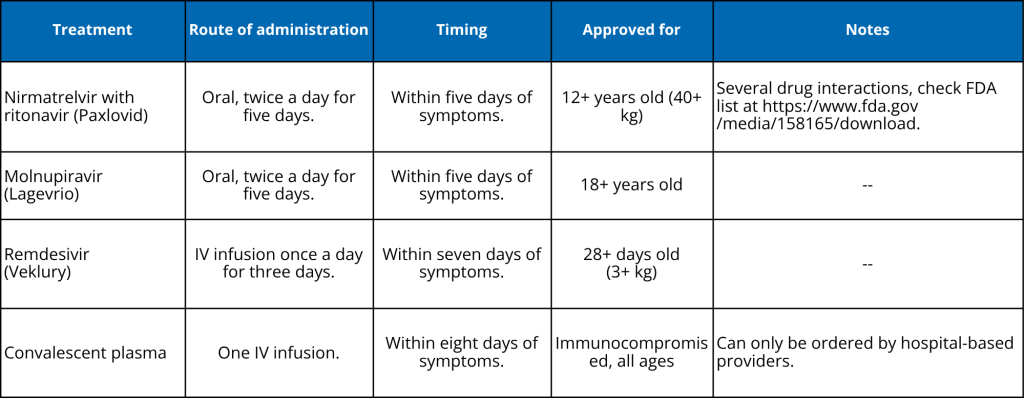
If you test positive for COVID-19 by either a rapid antigen test or a PCR test, contact your healthcare provider to get and start treatment as soon as possible. There are antiviral medications and convalescent plasma available to treat COVID-19, all of which are most effective within 5-8 days of the beginning of symptoms [15]. Nirmatrelvir with ritonavir (trade name Paxlovid) and remdesivir (trade name Verklury) are likely the most effective treatments to prevent severe COVID-19 and death.
Many people delay COVID-19 antiviral treatment because they don’t feel ‘that bad’ at first, but mild symptoms can rapidly become serious. Earlier treatment = better outcome!
The best way to prevent severe COVID-19 is to get vaccinated and keep up-to-date on boosters recommended by your healthcare provider. A study conducted through the USIDNET patient registry showed that vaccinated people with PI who had COVID-19 were significantly less likely to be hospitalized, be admitted to the ICU, or die than those with PI who were not vaccinated [16]. Household members of people with PI should get vaccinated to create a "protective cocoon" around the person with PI and decrease their exposure to the SARS-CoV-2 virus.
In March 2024, the U.S. Food and Drug Administration (FDA) authorized pemivibart (trade name Pemgarda) to prevent COVID-19 infections in those 12+ years old who are moderately to severely immunocompromised [17]. Pemgarda is a monoclonal antibody, which means that unlike vaccines, it provides protection regardless of how well a person’s immune system works. It is not approved for use after exposure or infection. Pemgarda is given as an intravenous infusion every three months and must be prescribed by a healthcare provider. Infectious Disease Society of America’s clinical guidelines for Pemgarda can help healthcare providers determine if their patients should receive it [18].
Respiratory syncytial virus (RSV)
In the U.S., RSV season typically lasts from October through April, with a peak in December or January. Symptoms include runny nose, coughing, sneezing, fever, and difficulty breathing. RSV has two subtypes, A and B, that differ genetically, but there is no difference in disease severity between them. Along with chronic heart and lung disease, being immunocompromised is a risk factor for developing severe RSV.
Research on RSV in those with primary immunodeficiency (PI) has primarily focused on infants and children. A 2012 paper found that children with PI are 3.8 times more likely to be hospitalized for an RSV infection than children without a chronic condition [19]. Studies in Japan and Spain found that, in particular, children with PIs that affect T cells (for example, combined immunodeficiencies) are at the greatest risk of hospitalization for RSV [20], [21].
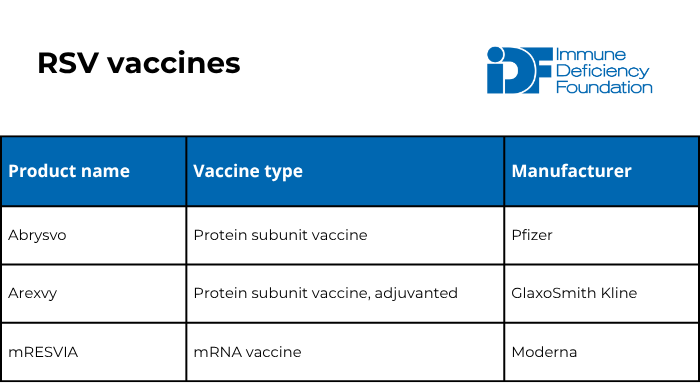
The FDA has approved five preventative products for RSV within the last couple of years: three vaccines and two long-lasting monoclonal antibodies. Unlike vaccines, monoclonal antibodies are a type of passive immunization that provide protection regardless of how well a person’s immune system works. Monoclonal antibodies work like immunoglobulin replacement therapy but only protect against one specific germ.
Infectious Diseases Society of America (IDSA) published recommendations on the prevention of respiratory syncytial virus (RSV) infection specifically in immunocompromised individuals. IDSA recommends that all individuals aged 18 years and older who are immunocompromised receive one dose of an RSV vaccine. In addition, the American Academy of Family Physicians (AAFP) recommends that pregnant individuals who have not received an RSV vaccine previously get vaccinated. These individuals should get one dose of the Abrysvo vaccine when they are 32-36 weeks pregnant from September through January.
Unlike the flu and COVID-19, experts consider RSV vaccination protective for a long period of time. There are currently no recommendations for any group to receive more than one dose in their lifetime.
The RSV vaccine is safe and cannot cause RSV in anyone, no matter how weak their immune system, because it does not contain live virus.
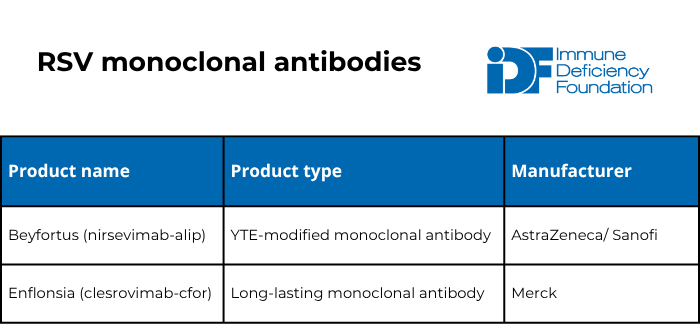
The American Academy of Pediatrics (AAP) recommends one dose of either of the two long-lasting monoclonal antibodies for:
- Babies 7 months old or younger born to individuals who have never been vaccinated for RSV or were vaccinated for RSV during a previous pregnancy.
- Babies 8-19 months old who are at high risk of severe RSV infection either because of a medical condition (including severe immunocompromise) or because of American Indian/Native Alaskan heritage.
Pneumonia
Pneumonia is an infection in the lungs that can be caused by many different types of germs but is usually caused by bacteria, such as Streptococcus pneumoniae (pneumococcus) or Mycoplasma pneumoniae, or respiratory tract viruses. However, certain PIs, like CD40 ligand deficiency or chronic granulomatous disease (CGD), make a person more likely to get pneumonia caused by unusual germs, including fungi like Pneumocystis jirovecii or Aspergillus spp.
Symptoms of pneumonia include chills, high fever, coughing, and chest pain when breathing or coughing. If you have these symptoms, you should see your healthcare provider for the proper diagnosis and treatment. It is important that your healthcare provider check for COVID-19 or influenza if you have pneumonia, as these infections need to be treated early with antiviral medications, not antibiotics. Fungal pneumonia also needs specific treatment and can be very serious if it is not diagnosed and treated quickly.
In addition, healthcare providers should consider that an underlying, undiagnosed PI may be present in people who have:
- Recurrent pneumonia, defined as two episodes of pneumonia within a year (with clear lungs on imaging tests in between) or three episodes of pneumonia in a lifetime [22].
- Unusually severe pneumonia without other risk factors.
- Pneumonia caused by an unusual germ like Pneumocystis jirovecii fungi.
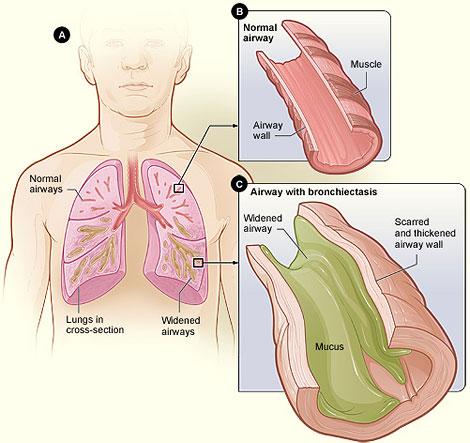
Bronchiectasis
Bronchiectasis is when the airways in the lungs become permanently wider, usually due to damage from recurrent infections in the airways. There are numerous medical problems that can lead to bronchiectasis including PIs. In people with bronchiectasis, it's hard to clear mucus and germs from the airways, which can lead to more frequent and severe pneumonia. A chronic cough that brings up mucus from the lower airways (sputum) is the most common symptom. Other symptoms include fatigue and shortness of breath.
The treatment of bronchiectasis depends on the cause, severity, and other features. Usually, a pulmonologist needs to be part of the team to properly treat this condition.
Preventing respiratory infections
There are several strategies that can help you avoid respiratory infections and stay well:
- Get vaccinated for both influenza and COVID-19, even if you are on Ig therapy. Also, talk to your immunologist about whether you should get vaccinated against other germs that can cause respiratory infections, such as RSV and Streptococcus pneumoniae.
- It’s important for household members or other close contacts to get vaccinated too!
- Regularly wash your hands with soap and water, especially after coughing or sneezing, after using the bathroom, and before eating.
- Hand sanitizer with at least 60% alcohol can also prevent infections when soap and water are not available. However, hand sanitizer does not kill some germs and may not be as effective as handwashing with soap and water when the hands are greasy or very dirty [24]. When using hand sanitizer, read the label for the correct amount of sanitizer to use and rub the entire hand until completely dry; do not wipe the sanitizer off before it has dried.
- Regularly disinfect high-touch surfaces in your home, like door knobs, sink handles, and light switches, especially during cold and flu season.
- Avoid individuals who are sick.
- Try not to touch your nose, mouth, or eyes, as germs can spread this way.
- Avoid crowded indoor areas such as shopping malls, restaurants, and movie theaters, especially during cold and flu season.
- During cold and flu season, use a well-fitted N95 or KN95 mask when out in public that completely covers your nose and mouth to avoid inhaling germs [25].
You can also prevent the spread of germs when you have a respiratory infection:
- When coughing or sneezing, cover your nose and mouth with a sleeve, elbow, or tissue. Dispose of the tissue after use.
- Stay home from work or school until you have been fever-free and your symptoms are improving for 24 hours. Take additional precautions, like wearing a mask and distancing from others, for five days.
Managing respiratory infections
Many different kinds of germs can cause infections in the respiratory system in people with PI. Respiratory infections can be as mild as a cold or as serious as pneumonia. There are antibiotics to treat infections caused by bacteria and antiviral medications for the flu or COVID-19. Home tests for influenza and COVID-19 can help you get diagnosed quickly so that your healthcare provider can prescribe these treatments.
However, treatment for most respiratory infections focuses on easing symptoms and preventing further problems. Your healthcare provider might suggest over-the-counter medicine to lower fever and relieve body aches. Other helpful medications include expectorants, which thin out mucus to make it easier to cough up, and decongestants, which reduce swelling of the mucous membranes in the nose and sinuses.
It's important to drink plenty of fluids to stay hydrated. Drinking different kinds of non-alcoholic drinks is helpful. Drinks with crushed ice or carbonation can soothe a sore throat. Warm drinks, like tea, can help clear nasal passages and ease chest tightness.
During the worst part of a respiratory infection, you may lose your appetite. This usually doesn't last long. Eating small, frequent meals of liquids and light foods is often effective. Once your appetite returns, your healthcare provider might recommend a diet high in calories and protein to replace what your body lost during the illness.
Other ways to feel better include:
- Rinsing your mouth with plain water regularly. This can help with dryness and the bad taste that often comes with being sick and breathing through your mouth.
- Using a vaporizer or humidifier to increase the moisture in the air and loosen mucus. If you use a vaporizer or humidifier, it's important to clean it daily to prevent mold.
- Applying petroleum jelly or lip balm to irritated skin on your lips and nose.
- Getting rest. If coughing or a runny nose keeps you from resting, try using extra pillows to raise your head and shoulders while you sleep. Sometimes, a cough suppressant can prevent coughing from waking you up at night.
This page contains general medical and/or legal information that cannot be applied safely to any individual case. Medical and/or legal knowledge and practice can change rapidly. Therefore, this page should not be used as a substitute for professional medical and/or legal advice. Additionally, links to other resources and websites are shared for informational purposes only and should not be considered an endorsement by the Immune Deficiency Foundation.
Adapted from the IDF Patient & Family Handbook for Primary Immunodeficiency Diseases, Sixth Edition.
Copyright ©2019 by Immune Deficiency Foundation, USA
Sign up for updates from IDF
Receive news and helpful resources to your cell phone or inbox. You can change or cancel your subscription at any time.
